Right bundle branch block (RBBB): ECG, criteria, definitions, causes & treatment
Right bundle branch block (RBBB)
Right bundle branch block (RBBB) is due to an anatomical or functional dysfunction in the right bundle branch, such that the electrical impulse is blocked. Figure 1 illustrates the components of the ventricular conduction system, including the right bundle branch (RBBB). In the presence of right bundle branch block, depolarization of the right ventricle relies on electrical impulses originating from the left ventricle. However, these impulses propagate slowly as they travel partially or entirely outside the specialized conduction system. This slow propagation leads to a delayed and abnormal activation sequence of the right ventricle, resulting in a prolonged and abnormal QRS complex on the ECG. The hallmark of right bundle branch block is QRS duration ≥0,12 seconds, large R’-wave in V1/V2 and a broad and deep S-wave in V5/V6.
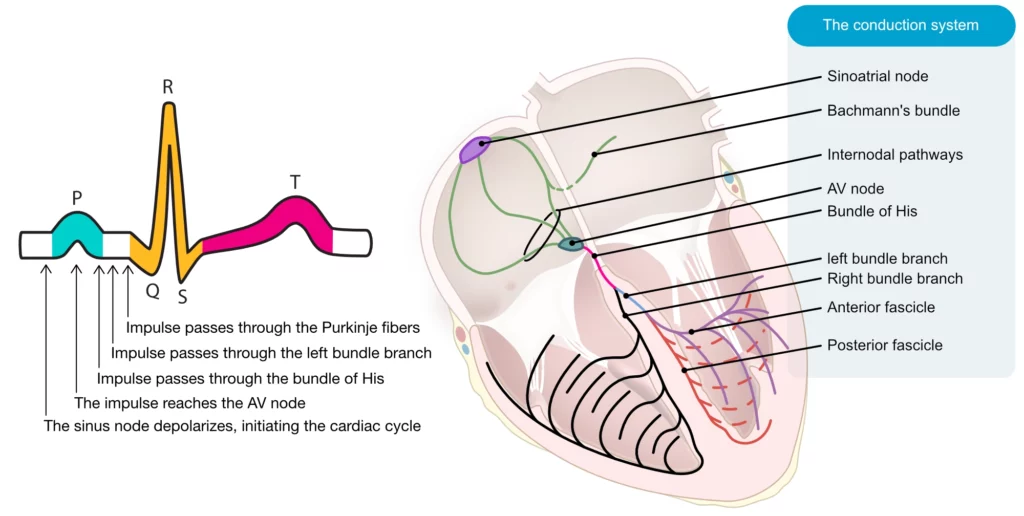
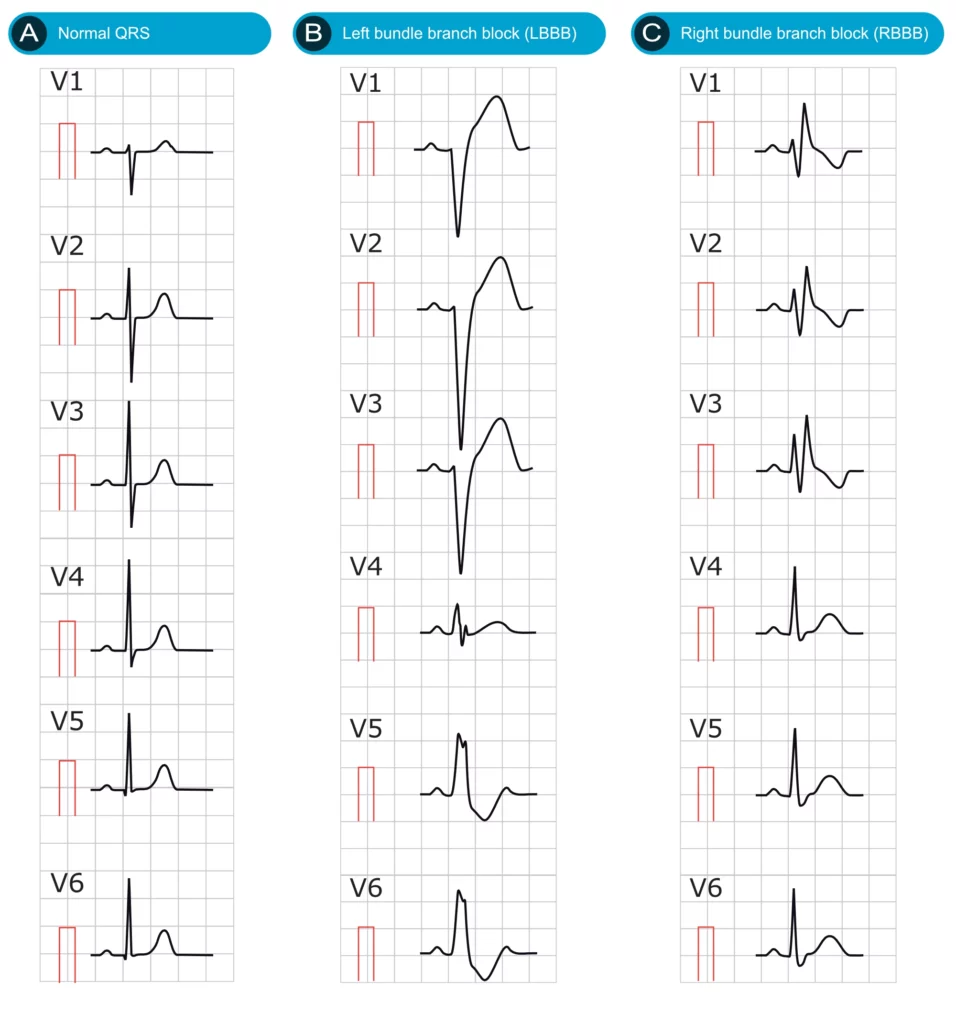
Figure 2 illustrates a normal ECG, a left bundle branch block (LBBB) and a right bundle branch block (RBBB).
ECG criteria for right bundle branch block (RBBB)
- QRS duration ≥0,12 seconds.
- Leads V1-V2: The QRS complex resembling the letter M. More specifically, the QRS complex displays rsr’, rsR’ or rSR’ pattern (rSR’ is the most common; Figure 2). Occasionally the S-wave does not reach the baseline. The second R-wave (denoted R’) is virtually always larger than the first R-wave.
- Leads V5, V6, I, aVL: Broad S-wave. S-wave duration is greater than R-wave duration, or S-wave duration is greater than 40 ms in V6 and I.
- ST-T changes: V1-V2 shows downsloping ST-segments and inverted T-waves. Leads V5, V6, I and aVL show positive T-waves.
If QRS duration is between ≥0,110 seconds and <0,12 seconds, the right bundle branch block is said to be incomplete. Note that a second r-wave (r’) may occur as a normal variant in lead V1 (the normal variant has a normal QRS duration). Moreover, the normal septal q-waves (seen in V5, V6) are not affected by the right bundle branch block. Occasionally, right bundle branch block only displays a broad and notched R-wave in V1 (instead of two R-waves); in that scenario, the R-wave peak time should be >0.05 seconds.
Figure 3 shows the distinguishing features of right and left bundle branch block in the precordial (chest) leads.
Log in to view image, video, quiz, text

Figure 4 shows morphological differences between LBBB and RBBB on 12-lead-ECG at paper speed 50 mm/s.
Log in to view image, video, quiz, text
Electrophysiology of right bundle branch block (RBBB)
Under normal conditions, both ventricles depolarize simultaneously. However, the QRS morphology is dominated by electrical vectors from the left ventricle due to its significantly larger mass compared to the right ventricle. In right bundle branch block (RBBB), the right ventricle depolarizes after the left ventricle, allowing its electrical vectors to become evident. These vectors manifest in the later part of the QRS complex as an R’ wave (pronounced “R prime”), which is directed anteriorly and rightward.
Due to the abnormal depolarization sequence of the right ventricle in RBBB, repolarization is also abnormal, leading to secondary ST-T changes, which appear on the ECG as discordant ST-T segments. These ST-T segments are directed opposite to the QRS complex. As illustrated in Figure 3, a positive QRS complex in lead V1 is accompanied by a negative ST-T segment, defined by ST-segment depression and T-wave inversion. Similar patterns are typically observed in lead V2 as well. However, RBBB does not cause secondary ST-T changes in V5-V6.
The electrical axis in right bundle branch block (RBBB)
Right bundle branch block does not affect the electrical axis of the heart. Axis deviation indicates that there is a concomitant fascicular block, or other abnormality. Left axis deviation suggests concomitant left anterior fascicular block. Right axis deviation suggests concomitant left posterior fascicular block.
Clinical significance of right bundle branch block
Prevalence of RBBB
The prevalence of right bundle branch block (RBBB) in healthy individuals varies by age, gender, and diagnostic criteria, ranging from 0.2% to 8% in the general population. Specifically, complete RBBB is observed in approximately 3.2%, while incomplete RBBB (iRBBB) accounts for 4.6%, leading to a combined prevalence of 8% for all forms of RBBB (Alventosa-Zaidin et al.). RBBB is more common in men than women; one study reported complete RBBB in 1.4% of men compared to 0.5% of women (Bussink et al.). The prevalence of complete RBBB increases with advancing age, reaching up to 11.3% in individuals aged 80 years or older.
Long-term prognostic implications of RBBB
While traditionally considered benign in asymptomatic individuals, recent evidence suggests that RBBB may be linked to an increased cardiovascular risk. The Copenhagen City Heart Study (1976–2003) analyzed 18,441 participants who were free from prior myocardial infarction, heart failure, or left bundle branch block, following them through 2009 for all-cause mortality and cardiovascular outcomes. The study found that right bundle branch block (RBBB) and incomplete RBBB (iRBBB) were more prevalent in men than women (1.4%/4.7% in men vs. 0.5%/2.3% in women). Key predictors of incident RBBB included male sex, older age, high systolic blood pressure, and the presence of incomplete RBBB. Complete RBBB was associated with increased all-cause mortality (1.3-fold higher relative risk) and cardiovascular mortality (1.9-fold higher relative risk), as well as an elevated risk of myocardial infarction (1.7-fold higher relative risk) and pacemaker implantation (2.2-fold higher relative risk). However, it was not associated with heart failure or atrial fibrillation. In contrast, incomplete RBBB was not associated with any adverse outcomes. The findings suggest that RBBB in asymptomatic individuals may signal increased cardiovascular risk, challenging the perception of its benign nature (Bussink et al.).
Important differential diagnoses in the emergency setting
Log in to view image, video, quiz, text
Causes of right bundle branch block (RBBB)
- Idiopathic fibrosis or degeneration in the right bundle branch
- Congenital heart disease
- Ischemic heart disease (coronary artery disease)
- Acute cor pulmonale (pulmonary embolism)
- Chronic obstructive pulmonary disease
- Cardiac surgery may cause permanent or transient RBBB
- PCI may cause transient RBBB
- Cardiomyopathy (particularly hypertrophic obstructive cardiomyopathy)
- Aberrant ventricular conduction (aberrancy)
Diagnosis of ischemia and infarction in the setting of RBBB
The right bundle branch block does not interfere with the diagnosis of ischemia/infarction. It is possible to diagnose pathological Q-waves (because the initial part of the QRS is not affected by the RBBB). Acute ischemia (ST-T changes) may also be judged as usual, despite the bundle branch block. Note that acute cor pulmonale with RBBB may cause large Q-waves in V1–V3, II, III and/or aVF.

