Atrial fibrillation: ECG, classification, causes, risk factors & management

Atrial fibrillation: definitions, causes, risk factors, ECG diagnosis and management
- Complications of atrial fibrillation and available treatments
- Symptoms of atrial fibrillation
- ECG in atrial fibrillation
- Classification of atrial fibrillation
- Arrhythmias associated with atrial fibrillation
- Mechanisms: atrial fibrillation begets atrial fibrillation
- Electrophysiological mechanisms of atrial fibrillation
- Examination of atrial fibrillation
- Management of atrial fibrillation
Atrial fibrillation is the most common abnormal tachyarrhythmia (only sinus tachycardia is more common). The prevalence of atrial fibrillation correlates strongly with age. Approximately 10% of individuals aged 80 years and above have atrial fibrillation, whereas the arrhythmia is unusual among persons younger than 50 years of age. The overall prevalence in a Western population is 1.0% to 1.5%. The crude prevalence is lower in non-Western countries, primarily due to the younger age-composition in those countries (adjusted prevalence figures are scarce). Indeed, the strongest risk factor for developing atrial fibrillation is age. Other significant risk factors are as follows: male sex, hypertension, left ventricular hypertrophy, left ventricular dysfunction, valve disease, coronary artery disease, cardiomyopathy, congestive heart failure, congenital heart disease, diabetes mellitus (both type 1 and type 2), obesity, smoking, obstructive sleep apnea and chronic obstructive pulmonary disease (COPD). Moreover, certain other tachyarrhythmias predispose to developing atrial fibrillation: atrial flutter, AVNRT and AVRT (pre-excitation, WPW syndrome) being the most common.
Atrial fibrillation with onset during hyperthyroidism (thyrotoxicosis), alcohol overdose, thoracic surgery, acute myocardial infarction, pericarditis/myocarditis or pulmonary embolism is often a reversible arrhythmia with low risk of recurrence. Atrial fibrillation in other circumstances (particularly those listed above) is usually a progressive disease.
Complications of atrial fibrillation and available treatments
In multivariable models (i.e statistical models in which adjustment has been made for confounders) individuals with atrial fibrillation are at five times increased risk of stroke and two times increased mortality, as compared with individuals without atrial fibrillation. The increased risk of stroke is explained by formation of thrombi in the left atrial appendage. Such thrombi may leave the appendage and enter the systemic circulation which causes thromboembolic occlusions of arteries in the brain, limbs or other organs. However, the increased risk in mortality is not completely explained by the increased risk of stroke; people with atrial fibrillation are at increased risk of cardiovascular mortality in general. This is not surprising given the adverse effects of long periods of tachycardia and desynchronized atrial and ventricular activity.
Fortunately, the treatment of atrial fibrillation has come a long way. Treatment with anticoagulation is highly effective in reducing stroke risk. Wrfarin and novel oral anticoagulants can reduce the risk of stroke by 70%, as compared with placebo. Besides anticoagulation, atrial fibrillation is treated with rate and/or rhythm control. Rate control implies the use of medications that slow ventricular rate (beta-blockers being the mainstay of this therapy). Rate control does not affect the rhythm per se. Rhythm control, on the other hand, attempts to restore sinus rhythm by use of antiarrhythmic drugs. Randomized controlled trials have not demonstrated any clear difference in mortality when comparing rate and rhythm control. However, rhythm control conveys risks (most antiarrhythmic drugs have a pro-arrhythmic effect as well), which is why clinicians mostly choose rate control. Both rate and rhythm control reduce morbidity, and mortality and improve quality of life. These approaches are discussed further below.
Symptoms of atrial fibrillation
Approximately 25% of all individuals with atrial fibrillation are asymptomatic (they have no symptoms). In such individuals, screening with ECG may reveal atrial fibrillation. Unfortunately, atrial fibrillation is too often discovered first at hospital admission due to its complications (stroke, thromboembolism, heart failure, dyspnea). Most individuals, however, do experience symptoms and they do so before developing complications. Symptoms such as palpitations, dyspnea, fatigue, chest/throat discomfort, and impaired exercise capacity are common and may all coexist. Dizziness is also common. Syncope, however, is uncommon. If a patient with atrial fibrillation experiences episodes of syncope or even pre-syncope, one must suspect tachy-brady syndrome, which implies that there is concomitant sinus node dysfunction. Atrial fibrillation debuting with congestive heart failure is uncommon among persons with previously normal left ventricular function.
Note that the tachyarrhythmia symptoms of atrial fibrillation (palpitations, chest discomfort, etc) occur abruptly. and patients typically report that the palpitations started suddenly.
ECG in atrial fibrillation
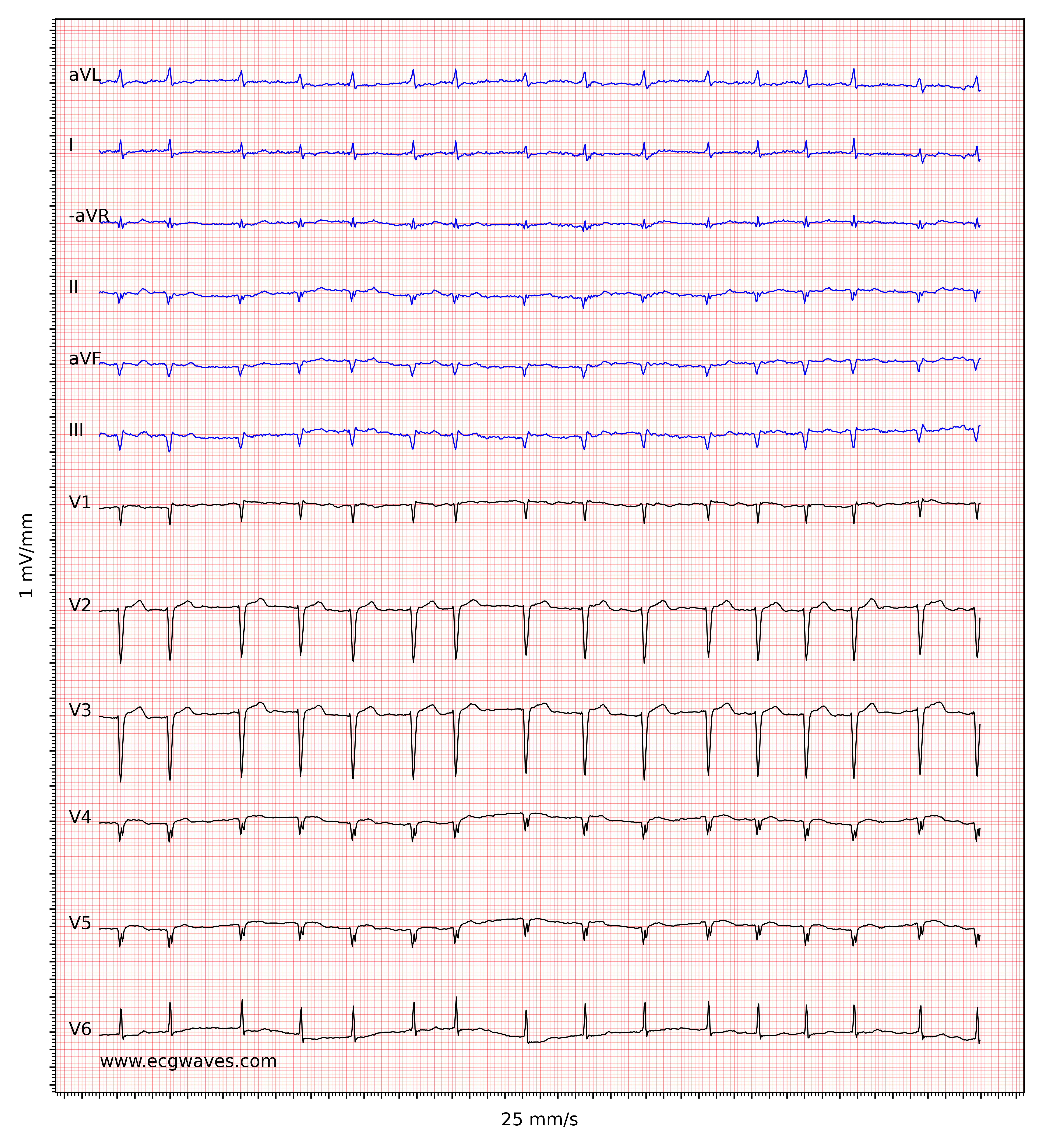

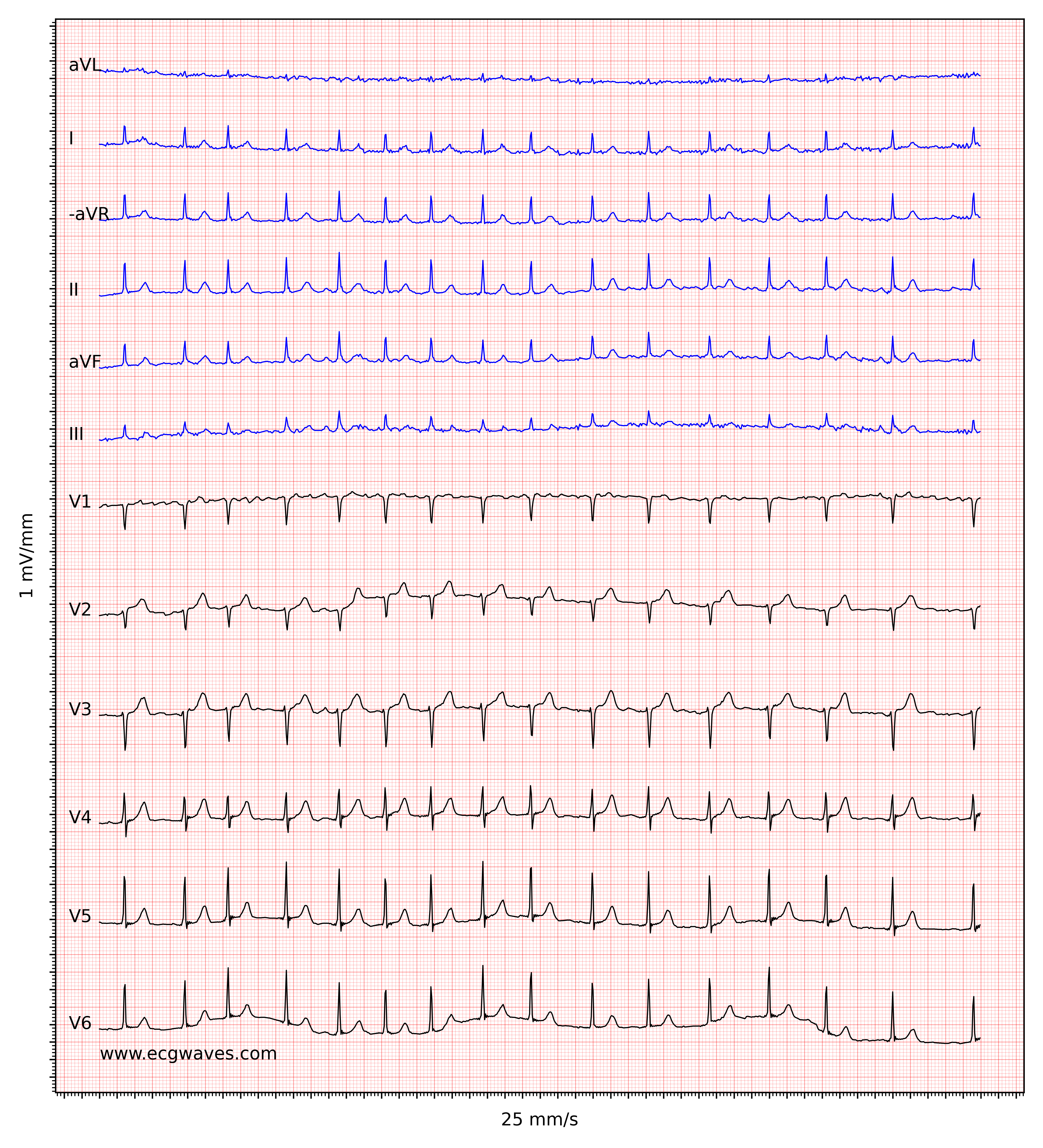

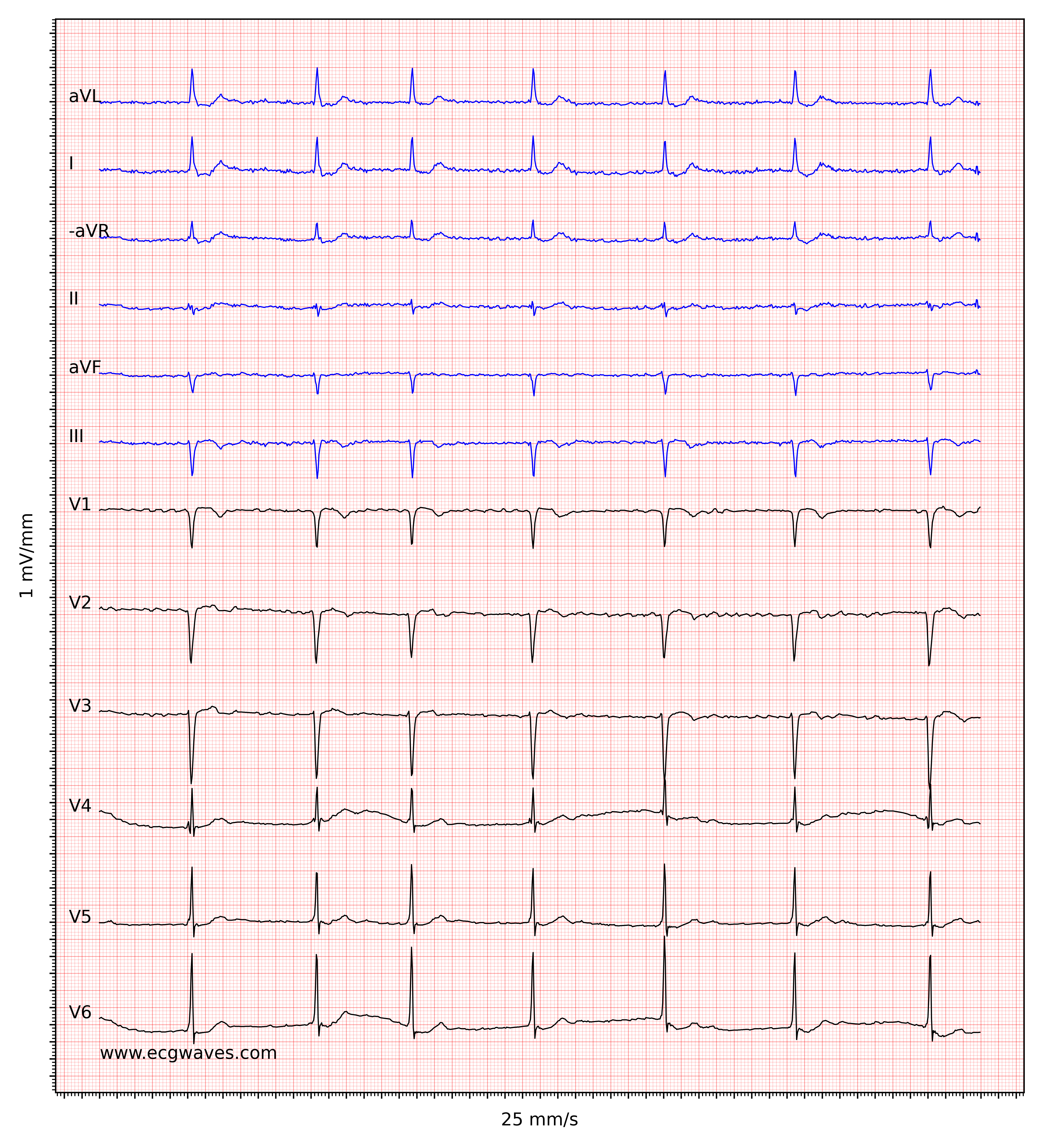
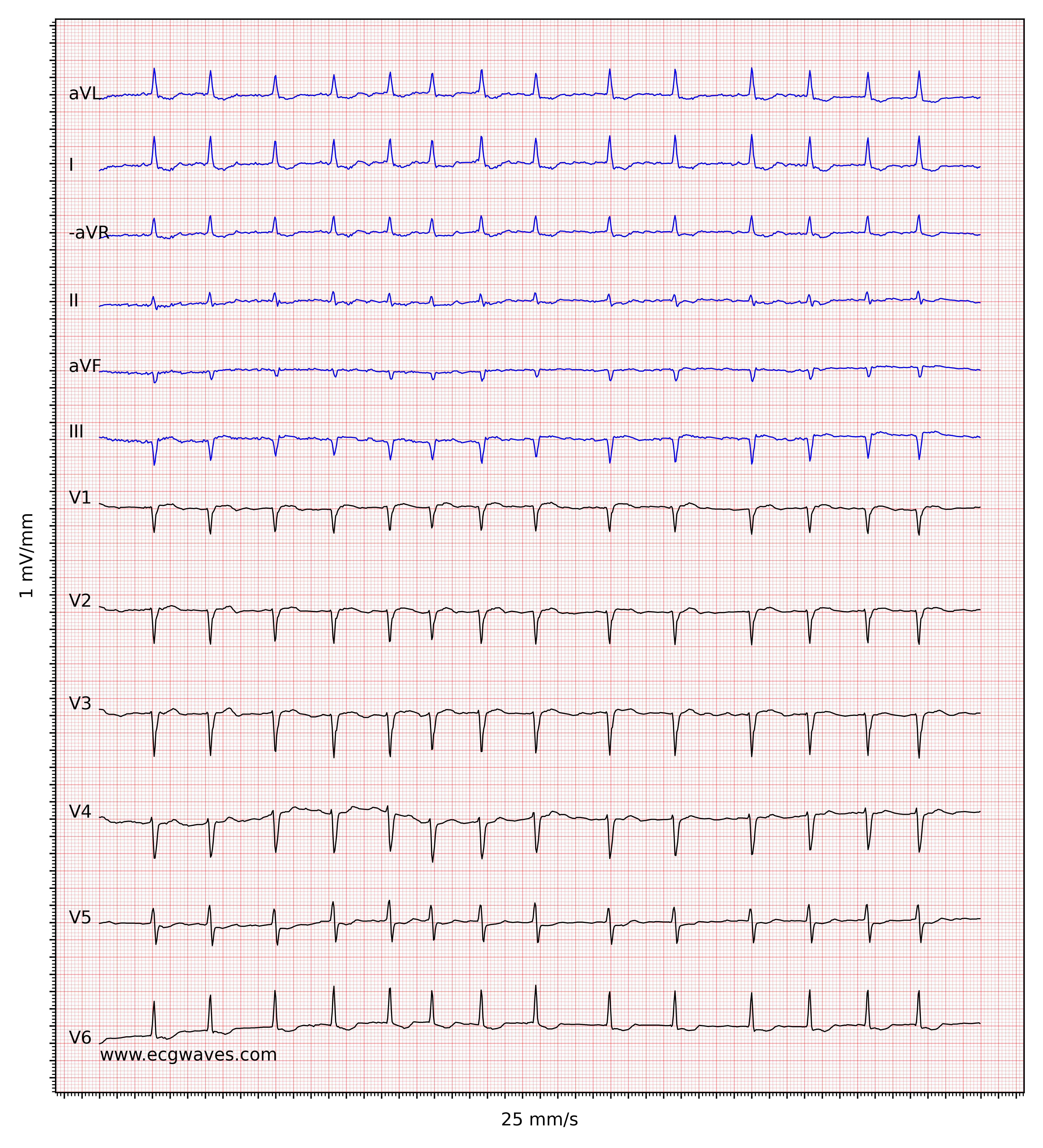

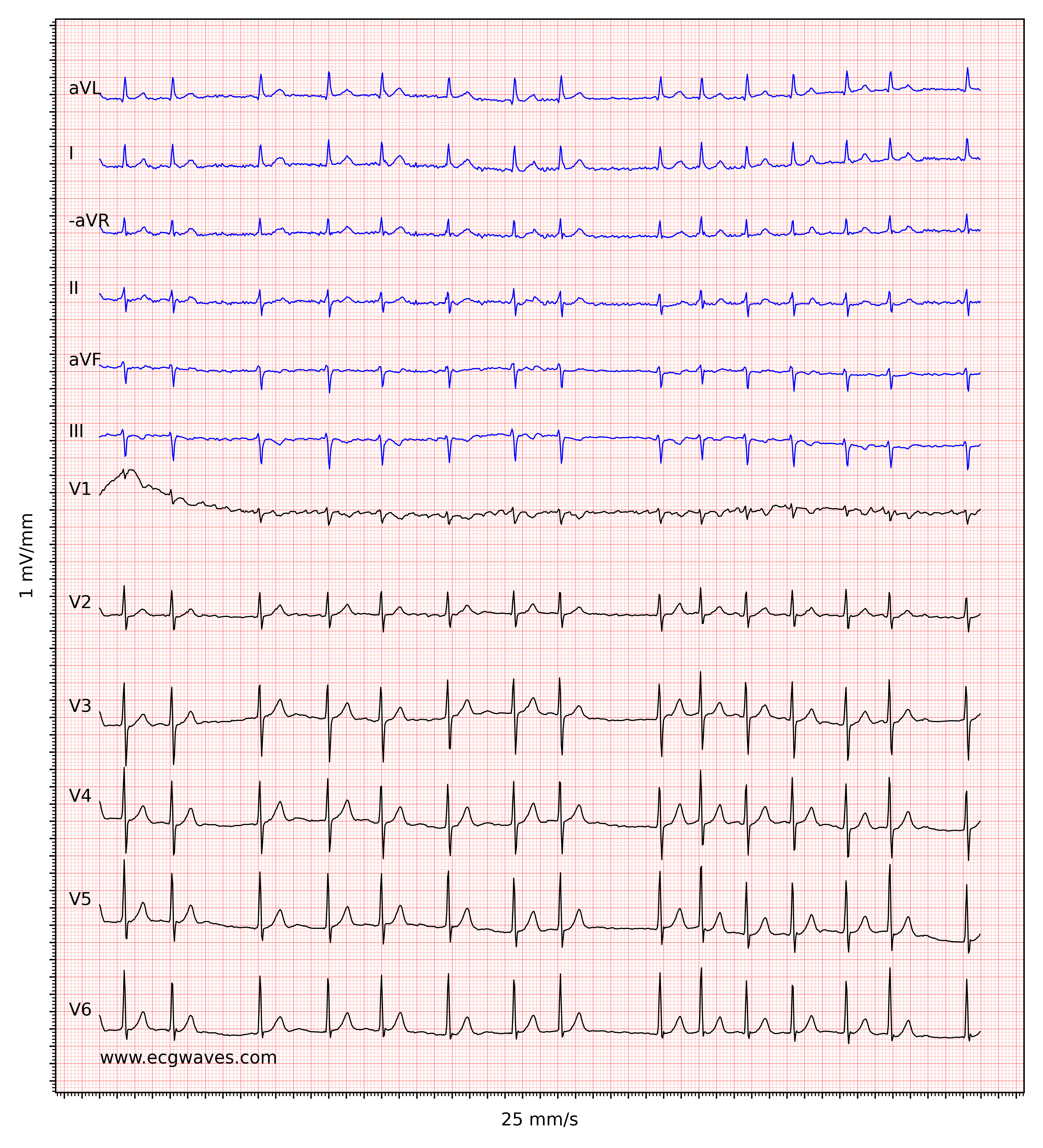
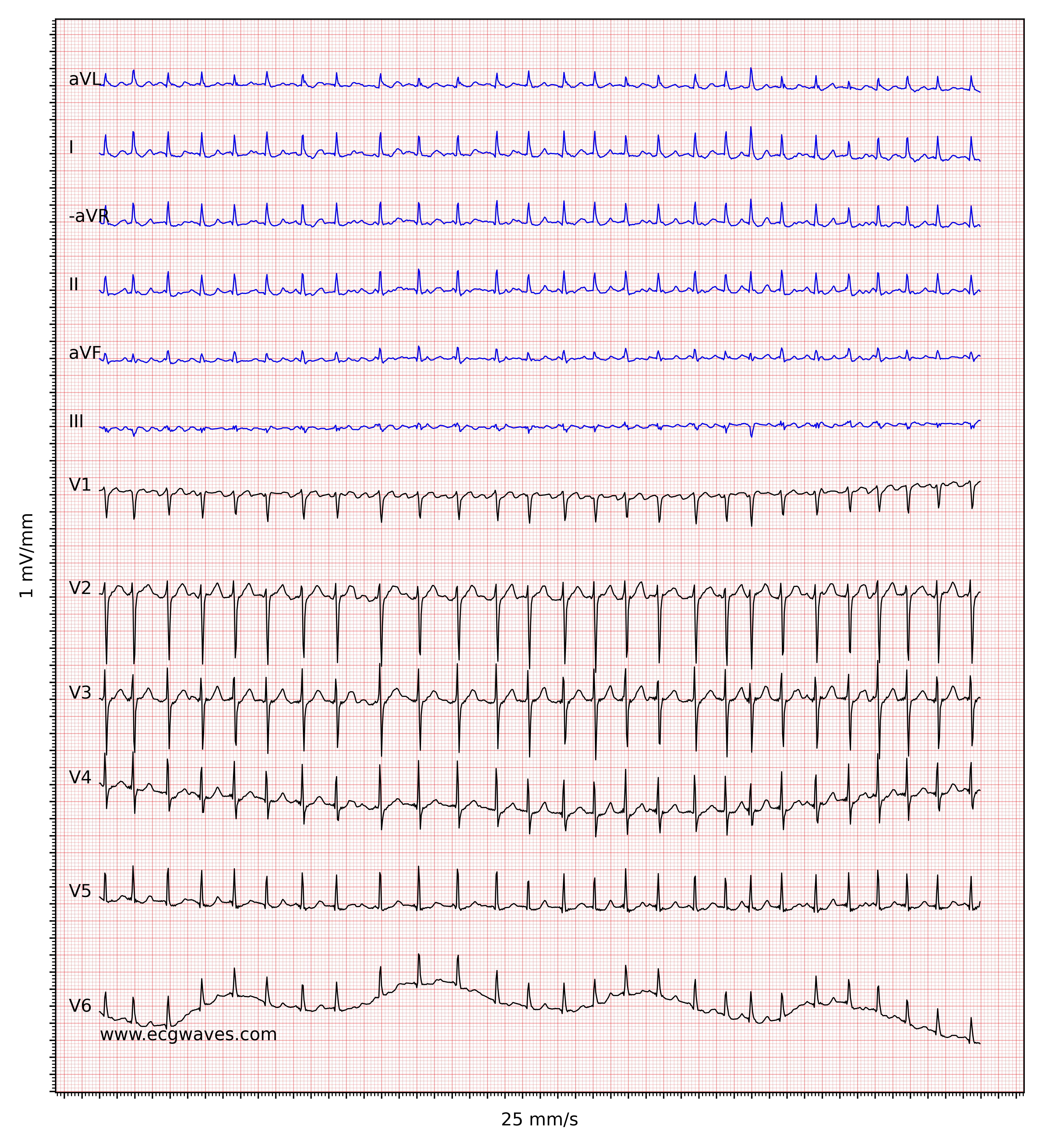
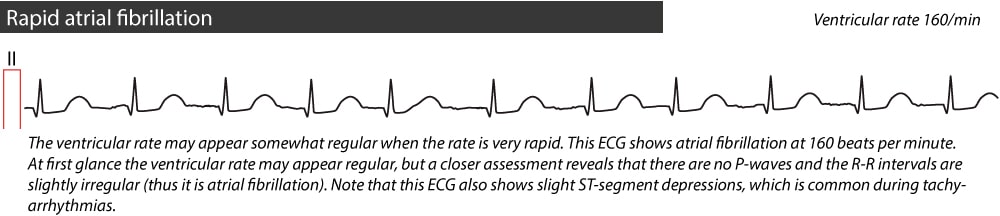
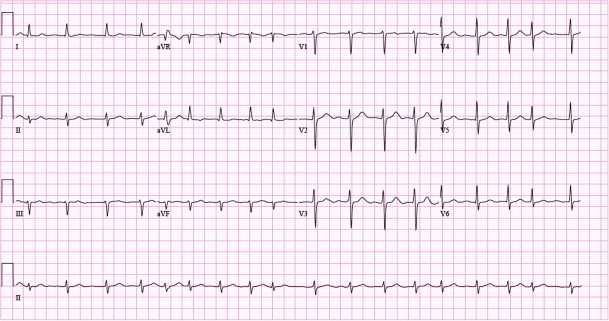
The hallmark of atrial fibrillation is the absence of P-waves and an irregularly irregular (i.e completely irregular) ventricular rate. The baseline (isoelectric line between QRS complexes) is characterized by either fibrillatory waves (f-waves) or just minute oscillations. Fibrillatory waves are small with varying morphology and high frequency (300 to 600 waves per minute). The amplitude of f-waves may vary from small to large. Large f-waves must not be mistaken for flutter waves (F-waves) which are seen in atrial flutter. It is, luckily, easy to distinguish these two because f-waves always show varying morphology whereas flutter waves are more or less identical (f-waves also have higher frequency than flutter waves). Figures 1 and 2 show ECG examples of atrial fibrillation.
Log in to view image, video, quiz, text

Log in to view image, video, quiz, text
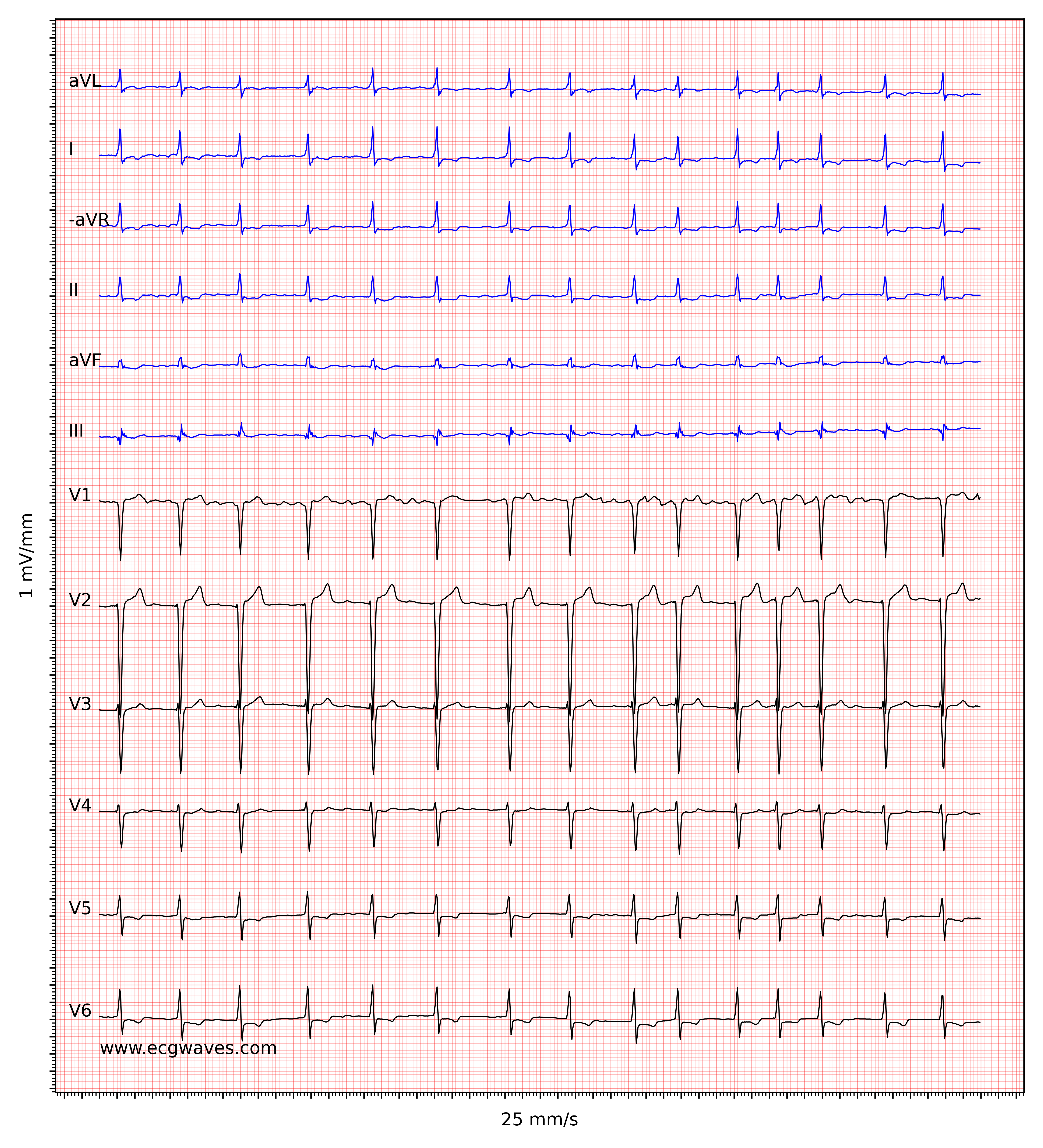
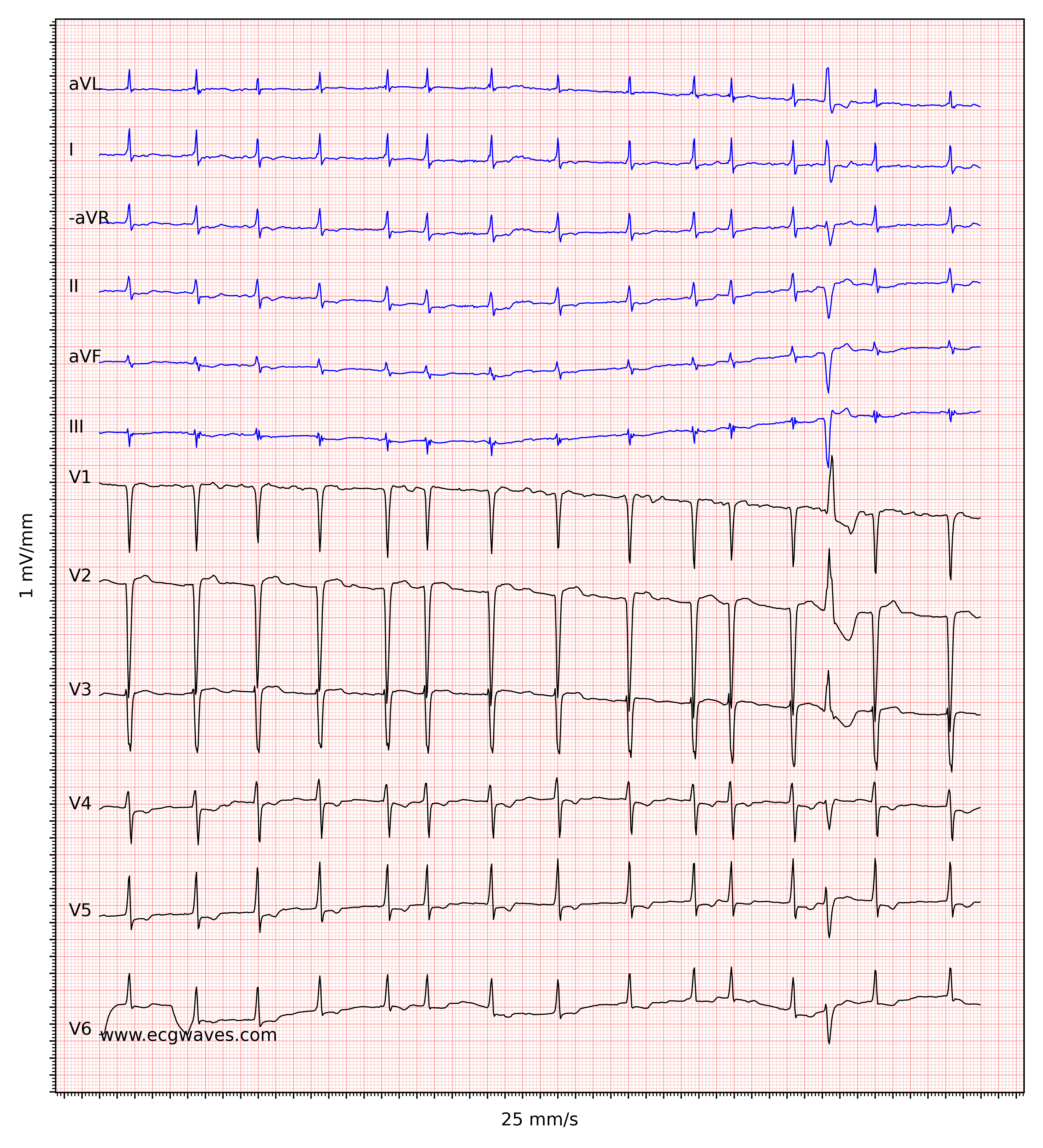
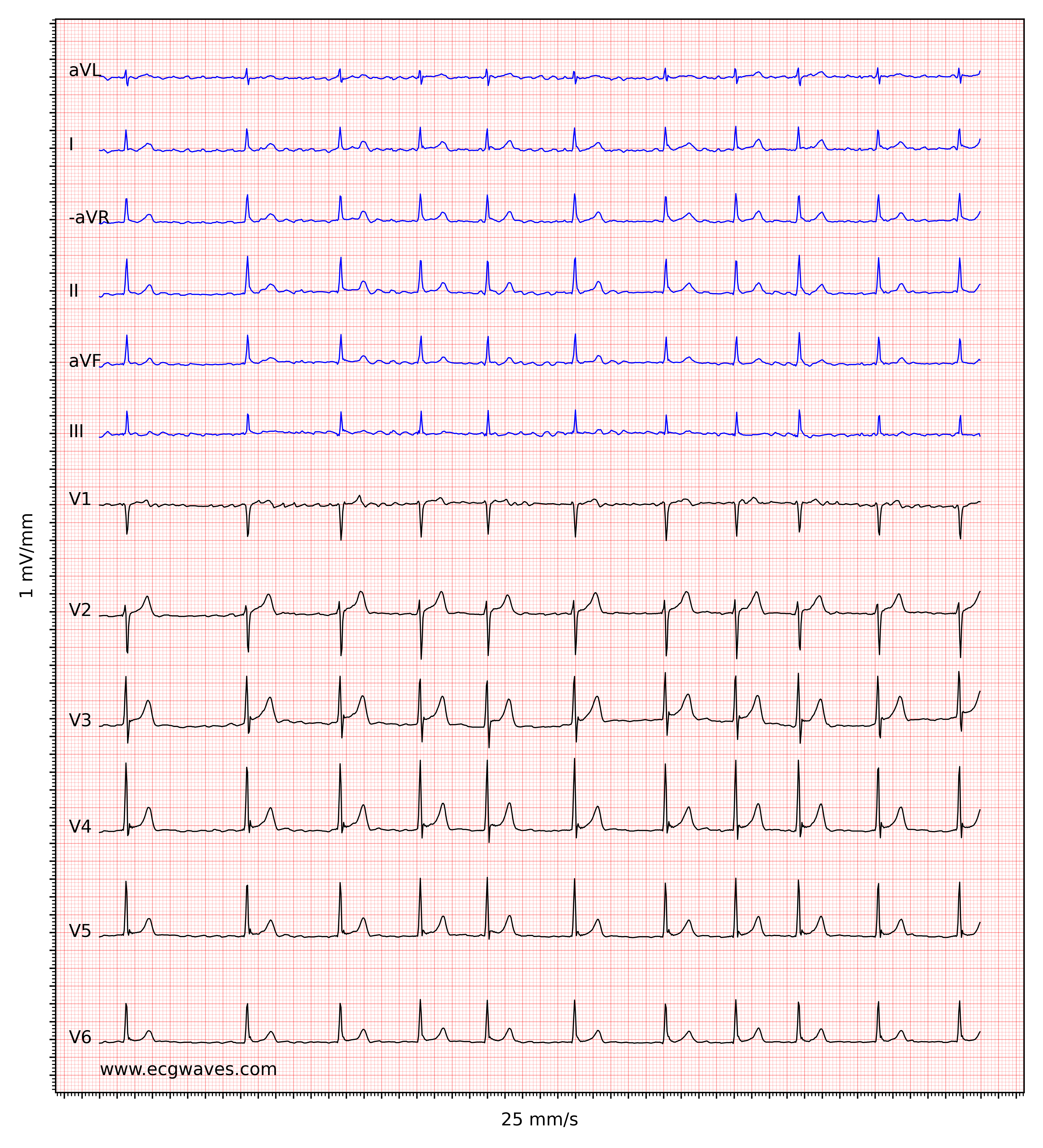
The ventricular rate is completely irregular, typically in the range of 100 to 180 beats per minute. Patient age, current medications, and concomitant AV blocks modify the ventricular rate. Atrial fibrillation with very rapid ventricular rate may appear as a regular rhythm (which is yet another reason to switch from 25 mm/s to 50 mm/s paper speed), which is why it is important to carefully measure the regularity of the rhythm. Refer to ECG in Figure 3. When in doubt, it is generally safe to apply carotid massage, which increases vagal activity to the atrioventricular node and thus increases blocking in the atrioventricular node; this lowers the ventricular rate and makes the irregularity more clear.
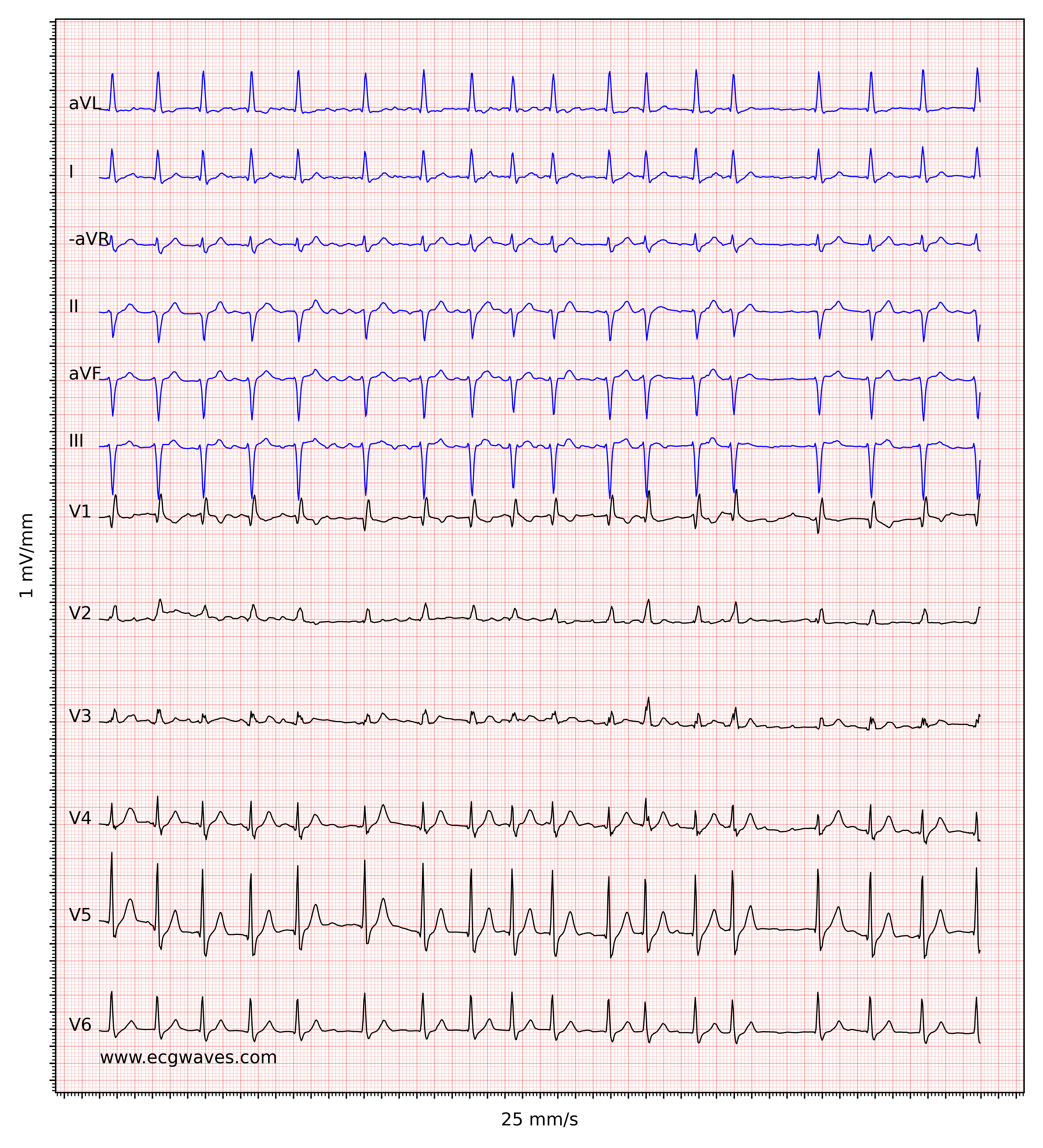
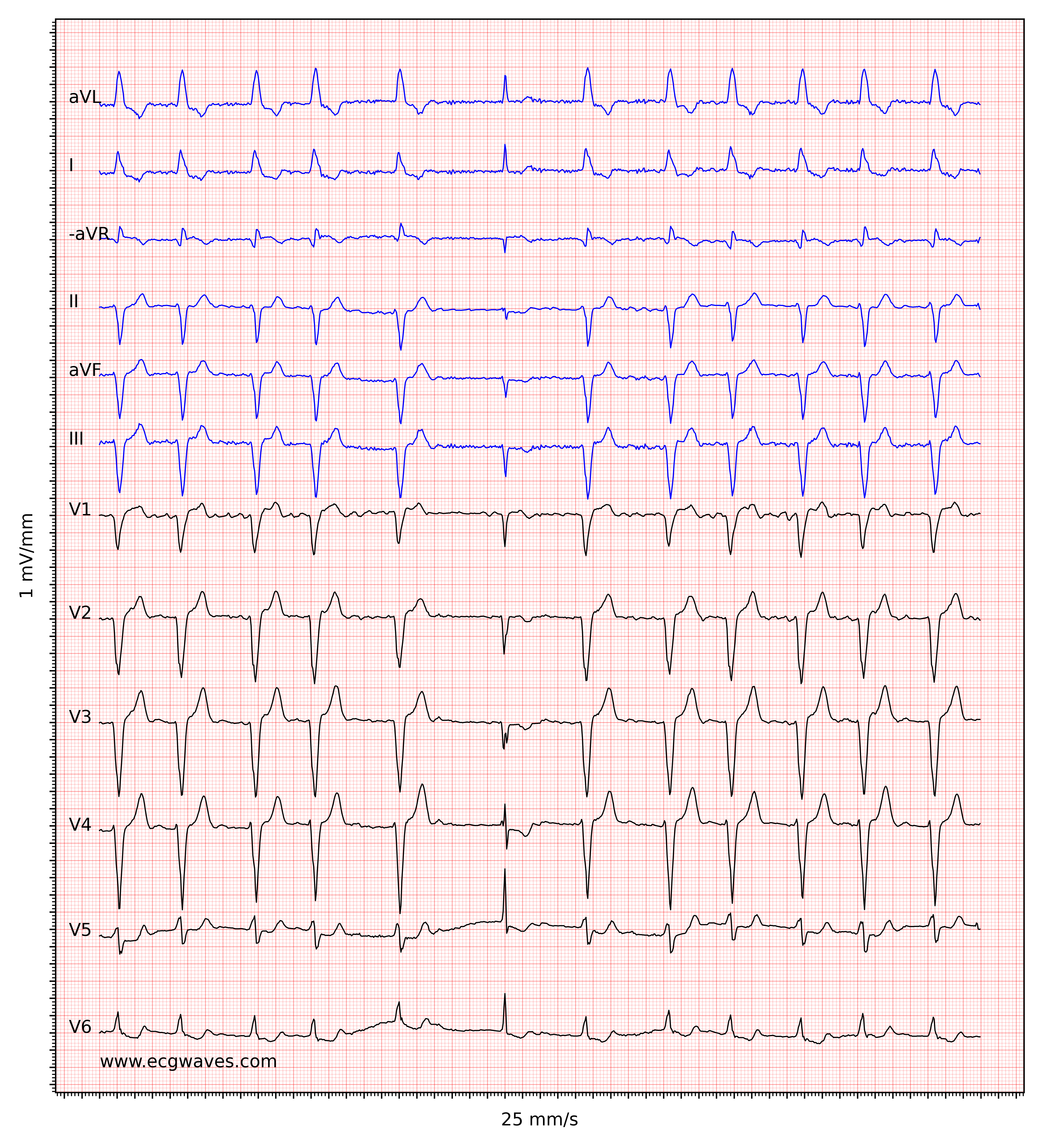
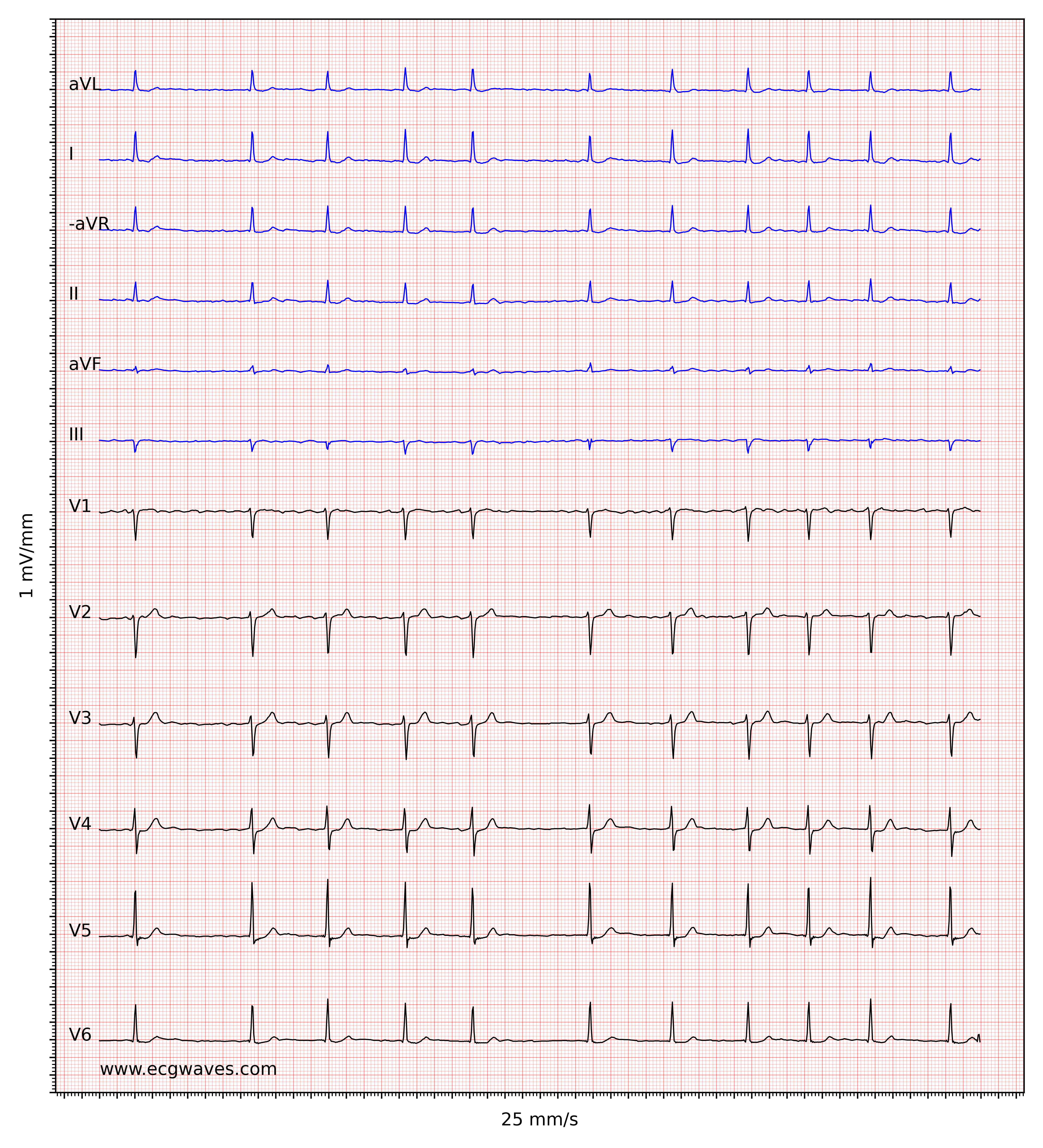
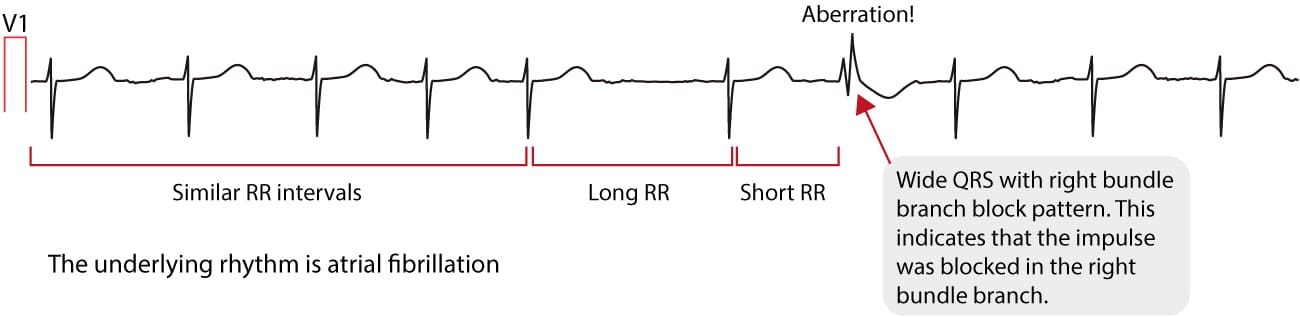
Atrial fibrillation and Ashman’s phenomenon
Atrial fibrillation does not affect the morphology of the QRS complex, provided that intraventricular conduction is normal. However, Ashman’s phenomenon is frequently seen in atrial fibrillation. Ashman’s phenomenon is a special type of aberrant ventricular conduction, in which a bundle branch block occurs as a result of an abrupt change in the length of the cardiac cycle. The ECG below shows an example of Ashman’s phenomenon.
Classification of atrial fibrillation
Atrial fibrillation is classified according to the duration of the arrhythmia.
- First diagnosed atrial fibrillation: Atrial fibrillation that has not been diagnosed before, irrespective of its duration and symptoms.
- Paroxysmal atrial fibrillation: Paroxysmal atrial fibrillation with duration less than 7 days. The arrhythmia is self-terminating in the vast majority of cases and it typically lasts less than 48 hours.
- Persistent atrial fibrillation: lasts more than 7 days and generally requires intervention to be terminated.
- Long-standing persistent atrial fibrillation: continuous atrial fibrillation lasting more than 12 months.
- Permanent atrial fibrillation refers to a situation where both the patient and clinician have agreed to accept the condition, typically after numerous attempts to induce cardioversion, and have discontinued efforts to restore sinus rhythm. This decision may be revisited if the patient and clinician wish to make another attempt to restore sinus rhythm.
Whether the arrhythmia converts to sinus rhythm spontaneously or through cardioversion (electrical or pharmacological) does not affect the classification. However, electrical and pharmacological cardioversion does limit the natural duration of the arrhythmia and may therefore affect the classification.
Atrial fibrillation is typically a progressive disease that usually evolves towards permanent atrial fibrillation. This is generally a stepwise process in which persons with paroxysmal atrial fibrillation tend to have an increasing number of episodes until the arrhythmia is persistent. Once persistent, the number of episodes with persistent atrial fibrillation tends to increase until the arrhythmia is long-standing persistent. It should be noted, however, that some patients have paroxysmal or persistent atrial fibrillation throughout their disease course, while others never return to sinus rhythm after a first diagnosis.
Treatment with ablation is only meaningful in paroxysmal or persistent atrial fibrillation. Treatment with anticoagulants, rate control, or rhythm control should be considered in all types of atrial fibrillation.
Other types of atrial fibrillation
The term lone atrial fibrillation is used to describe a patient younger than 60 years of age, who does not have any other concomitant heart diseases or risk factors, and whose echocardiographic examination is normal. This type of atrial fibrillation has a good prognosis and generally does not require anticoagulation therapy.
The terms “valvular” and “non-valvular” atrial fibrillation are used to distinguish whether the atrial fibrillation is potentially secondary to valvular disease. This distinction has therapeutic implications, as valvular atrial fibrillation is significantly more challenging to convert to sinus rhythm. Attempting to cardiovert valvular atrial fibrillation is generally not considered effective, as most cases relapse into atrial fibrillation shortly after cardioversion, if the procedure is successful at all.
Arrhythmias associated with atrial fibrillation
Patients with atrial fibrillation frequently present with atrial flutter and/or atrial tachycardia. Individuals with pre-excitation (Wolff-Parkinson-White syndrome) are at high risk of developing atrial fibrillation. Some studies suggest that up to 30% of patients with clinically overt pre-excitation develop atrial fibrillation.
Mechanisms: atrial fibrillation begets atrial fibrillation
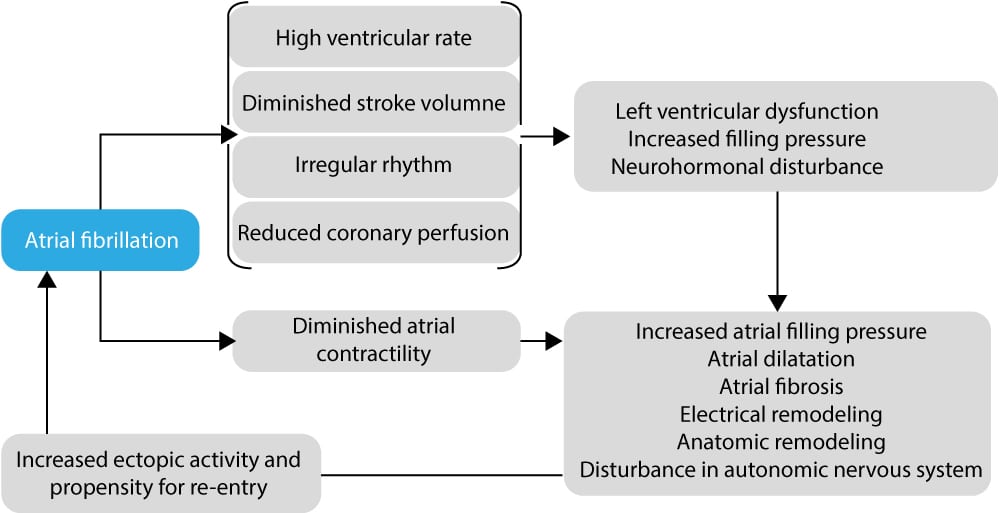
A large body of evidence demonstrates that atrial fibrillation in itself causes hemodynamic and electrophysiological changes in the myocardium which lead to increased susceptibility to new episodes of atrial fibrillation. Frequent and long-standing episodes of atrial fibrillation can thus create the prerequisites necessary for new episodes to emerge. These changes are illustrated in Figure 5. Ultimately, the anatomic and electrophysiological changes will lead to permanent atrial fibrillation (as explained below).
Electrophysiological mechanisms of atrial fibrillation
The short story
The anatomic and electrophysiological mechanisms causing atrial fibrillation are still under investigation. The underlying mechanisms are somewhat complicated (discussed in detail below). For those not interested in electrocardiology, it is sufficient to know that atrial fibrillation is caused by electrical chaos in the atria. The chaos is due to the simultaneous existence of multiple re-entry circuits that generate impulse waves that propagate through the atria. These impulse waves collide with each other and with refractory cells, which fragments the waves and causes additional chaos. Interested readers may continue to read the detailed explanation of this.
The long story
Atrial fibrillation is dependent on two mechanisms: a trigger and a driver. The trigger is the event that initiates the atrial fibrillation and the driver is the mechanism that will maintain the arrhythmia. The atria in individuals who develop atrial fibrillation display electrophysiological and anatomical properties that promote triggers and drivers. Aging, the strongest risk factor of atrial fibrillation, leads to degeneration of the myocardium and conduction cells. Other risk factors, such as structural heart disease (cardiomyopathy, heart failure, valvular disease), ischemic heart disease, pulmonary disease, genetic predisposition, autonomic dysfunction, etc, are other risk factors that promote triggers and drivers. Studies unambiguously show that most triggers and drivers arise from the pulmonary veins that empty oxygenated blood into the left atrium.
The transition between pulmonary veins and atrial myocardium appears to be electrically vulnerable and studies show that the majority of patients with paroxysmal atrial fibrillation have a trigger by a pulmonary vein. The trigger is composed of an ectopic focus which discharges impulses at a high rate. These impulses may induce short bursts of atrial fibrillation but unless a driver is established, the fibrillation will cease once the trigger stops discharging impulses. A driver may be established if the impulses spreading from the trigger encounter myocardium with varying conductivity or excitability. When the impulse encounters an area with varying conductivity/excitability, re-entry may arise due to blocking of the impulse. New impulse waves will spread from the re-entry and these waves may collide with other impulse waves and either be terminated or encounter new blocks which fragment the impulse. Fragmentation of the impulse will cause its remnants to spread in a random fashion through the atria. To sum up, paroxysmal atrial fibrillation is initiated by a trigger that discharges impulses at high frequency; impulses may encounter myocardium with heterogeneous or varying conductivity/excitability which may act as a block that gives rise to re-entry circuits. These re-entry circuits beget additional re-entry circuits.
Early phases of atrial fibrillation (i.e paroxysmal and newly diagnosed atrial fibrillation) are characterized by featuring one or a few ectopic foci. Such focus or foci can be localized and eliminated by means of ablation therapy. This is generally a cure for atrial fibrillation because elimination of the trigger will remove the initial cause. However, the number of ectopic foci and the number of generated re-entry circuits increase gradually as time goes and this correlates strongly with progression to persistent and long-standing persistent atrial fibrillation. For the same reason, ablation therapy is less effective in persons with persistent or long-standing persistent atrial fibrillation.
The explanation for the fact that the number of ectopic foci and re-entry circuits increase is because the atrial fibrillation (and the risk factors accompanying it) induce electrophysiological and anatomical changes in the atria and these changes promote triggers and drivers. This gradual evolution of atrial myocardium is referred to as atrial remodeling. The degree of atrial remodeling correlates strongly with the number of episodes of atrial fibrillation. Among the changes in the atria are, for example, changes in the expression and function of ion channels (particularly calcium channels) and the development of fibrosis. Ultimately the functional and anatomical structure of the atria becomes so remodeled that the atrial fibrillation becomes permanent.
Besides the pulmonary veins, ectopic foci may be located by the entry of the superior vena cava, inferior vena cava, the coronary sinus, and the attachment of Marshall’s vein.
The autonomic nervous system appears to have an important role in inducing paroxysmal atrial fibrillation. One-third of all individuals with paroxysmal atrial fibrillation experience their episodes in situations with high vagal activity (during sleep, at rest, or high sympathetic activity (during exercise, stress, etc). The autonomic nervous system modifies the action potentials in the atrial myocardium, particularly around the pulmonary veins. However, the autonomic innervation of the atria is not homogenous (the spread of autonomic fibers in the atria varies) which means that the effect on the action potentials is also not homogenous and this promotes atrial fibrillation.
Although atrial fibrillation is triggered by an ectopic focus in most cases, it may also be triggered by other arrhythmias such as AVRT or atrial flutter or even bradycardia. The latter (bradycardia) is believed to cause atrial fibrillation because at low heart rates, ectopic focuses may come to express themselves when they are not suppressed by the sinoatrial node.
Examination of atrial fibrillation
Atrial fibrillation is confirmed through various electrocardiographic methods, including resting ECG, Holter ECG, and event recorder. Holter ECG is particularly useful for assessing the frequency and duration of arrhythmia episodes, including asymptomatic episodes. The diagnostic criteria for atrial fibrillation based on electrocardiographic findings are as follows:
- Atrial fibrillation present throughout the entire 12-lead resting ECG recording.
- Atrial fibrillation lasting more than 30 seconds on Holter ECG or event recorder.
If coronary artery disease is suspected, myocardial perfusion imaging (SPECT or PET) or coronary CT angiography should be considered.
The following blood tests should be conducted for all patients: hemoglobin, sodium, potassium, creatinine, estimated glomerular filtration rate (eGFR), calcium, liver enzymes, PK-INR, APTT, lipid profile, glucose, HbA1c, thyroid-stimulating hormone (TSH), and T4 levels.
Echocardiography is recommended for all patients with newly diagnosed atrial fibrillation.
NT-pro-BNP levels may be measured if heart failure is suspected.
Management of atrial fibrillation
Treatment of acute atrial fibrillation
• Avoid attempting cardioversion in patients with severely compromised left ventricular ejection fraction. Converting to sinus rhythm in such patients can lead to a lower heart rate and a significant reduction in cardiac output, potentially resulting in cardiogenic shock.
• For patients not on anticoagulants or those receiving sub-therapeutic doses, previous guidelines recommended a 48-hour window for attempting cardioversion. However, in 2024, the European Society of Cardiology (ESC) revised this recommendation, shortening the window to a maximum of 24 hours for attempting cardioversion.
Approximately 60% of cases of acute atrial fibrillation will convert spontaneously to sinus rhythm within 16 hours from the onset of symptoms. If there are no signs of circulatory compromise one may expect the situation for 24 hours (counting from symptom onset) until cardioversion is attempted. If one plans performing cardioversion it must be done within 24 hours from symptom onset. Cardioversion is contraindicated after 24 hours due to the high risk of thromboembolism (unless a transesophageal echocardiogram can be performed to rule out thrombus formation in the atria (left atrial appendage). Electrical cardioversion is the most effective method, yielding a success rate of >90% with biphasic shock ≥120 J. Pharmacological cardioversion (flecainide, propafenone, ibutilide, amiodarone, vernakalant) is less effective (approximately 75% success rate) and these antiarrhythmic drugs may cause arrhythmias as well as circulatory compromise due to negative inotropic effect. Nevertheless, in any arrhythmia, electrical cardioversion is the safest treatment alternative.
Repeated administration of intravenous beta-blockers, digoxin or calcium channel blockers may be needed to lower ventricular rate. It is wise to start with beta-blockers and then, if beta-blockers are insufficient, administer digoxin.
One must immediately address whether the patient is in need of anticoagulants, and most patients should be admitted with a dose of low-molecular-weight heparin (LMWH) until a decision has been made regarding anticoagulation.
Long-term treatment of atrial fibrillation
Rate control of atrial fibrillation (control of ventricular rate)
The rapid ventricular rate during atrial fibrillation is one of the main causes of the increased mortality observed in individuals with atrial fibrillation. Rate control implies that the ventricular rate is the treatment target. The aim is to slow the ventricular rate as much as possible without provoking excessive bradycardia. Rate control is accomplished with medications that affect the AV node; more specifically these drugs slow conduction through the AV node and this results in fewer atrial impulses being conducted to the ventricles. Beta-blockers (propranolol, metoprolol, atenolol, esmolol, nadolol), calcium channel blockers (diltiazem, verapamil) and digoxin (digitalis) are excellent choices to lower ventricular rate. Sotalol is reserved for cardiologists, as it has pro-arrhythmic effects as well. Rate control is not inferior to rhythm control in terms of survival. Aiming at a ventricular rate below 100 beats per minute can be recommended. Details on medications and dosages follow in Table 1.
Rate control of atrial fibrillation: medications that slow conduction through the AV node
| MEDICATION | ADVANTAGES | DISADVANTAGES | DOSAGE | ONSET OF ACTION | ELIMINATION HALF-LIFE |
|---|---|---|---|---|---|
| BETA-BLOCKERS | |||||
| Propranolol | Rapid onset of effect, short durations of effect for IV forms; heart rate control at rest and with activity; oral forms available with varying durations of effect | May worsen heart failure in decompensated patient; may exacerbate reactive airway diseases; may cause fatigue, depression; abrupt withdrawal may cause rebound tachycardia, hypertension | • IV: 1 mg given as bolus, repeat q5min as needed to achieve goal • Oral: 10-30 mg/dose q6-8hr | • IV: onset of action within 5 min • Oral: onset of action within 1-2 hr | • IV: duration of effect is 30-60 min • Oral: 3-5 hr |
| Metoprolol | Same as propranolol. | Same as propranolol. | • IV: 2.5-5 mg over 2-3 min, repeat q5min as needed to achieve goal • Oral: 12.5-100 mg/dose q6-8hr • Sustained-release preparations available for once-daily dosing | • IV: onset of action within 5 min • Oral: onset of action within 1-2 hr | • IV: duration of effect is 30-60 min • Oral: 3-6 hr |
| Atenolol | Same as propranolol. | Same as propranolol. | • IV: 5 mg over 5 min, repeat q10min to achieve goal • Oral: 25-100 mg/dose q8-12hr | • IV: onset of action within 5 min • Oral: onset of action within 1-2 hr | • IV: duration of effect is 30-60 min • Oral: 6-9 hr |
| Esmolol (intravenous only) | Same as propranolol. | Same as propranolol. | • IV: 500 µg/kg over 1 min, then maintenance dose of 25-300 µg/kg/min; titrate by 25-50 µg/kg/min q5-10min to achieve goal | • IV: onset of action within 5 min | N/A |
| Nadolol (oral only) | Same as propranolol. | Same as propranolol. | • Oral: 40-80 mg daily initially; increase to 240-320 mg daily as needed to achieve goal; can be given once daily | • Oral: onset of action within 1-2 hr | 14-24 hr |
| CALCIUM CHANNEL BLOCKERS | |||||
| Diltiazem | Same as for beta blockers | May worsen heart failure in decompensated patient; may cause fatigue; abrupt withdrawal may cause rebound tachycardia, hypertension | • IV: 0.25 mg/kg over 2 min, then infusion at 5-15 mg/hr for up to 24 hr; repeat bolus of 0.35 mg/kg may be necessary • Oral: 30-120 mg/dose q6-8hr; sustained-release preparations available as once- or twice-daily doses | • IV: onset of action within 5 min • Oral: onset of action of 1 hr | 5-7 h |
| Verapamil | Same as for beta blockers | May worsen heart failure in decompensated patient; may cause fatigue; abrupt withdrawal may cause rebound tachycardia, hypertension | • IV: 5- to 10-mg bolus q15-30min to achieve goal • Oral: 80-120 mg dose q8-12hr; sustained-release preparations available as once- or twice-daily doses | • IV: onset of action within 5 min • Oral: onset of action of 1 hr | 5-12 h |
| OTHER | |||||
| Digoxin (digitalis) | Can be used in patients with heart failure | Slow onset of action; poor control of heart rate with activity; narrow therapeutic margin; long duration of effect | IV loading dose of up to 1.0 mg in first 24 hr, with bolus of 0.25-0.5 mg IV push; then remainder in divided doses 16-8hr; maintenance oral dose, 0.125-0.25 mg qd | • IV: up to 30 min • Oral: 2-4 hr | 36 hr |
Note that these medications may cause bradycardia, which may ultimately require consideration of other measures, such as catheter ablation of the AV node (discussed below).
Rhythm control of atrial fibrillation
Rhythm control means attempting to restore sinus rhythm. This is done by means of anti-arrhythmic drugs (sotalol, flecainide, propafenone, amiodarone, disopyramide, dronedarone). Rhythm control may be considered although most patients will relapse within one year and it does not provide a survival benefit as compared with rate control.
Catheter ablation
Ablation is a highly effective treatment for paroxysmal atrial fibrillation. There are usually one or a few ectopic foci that can be localized and eliminated with ablation therapy. Approximately 70% of paroxysmal atrial fibrillation cases may be cured with ablation therapy. Persistent atrial fibrillation has a more complex arrhythmia mechanism (more ectopic foci, more re-entry circuits spread throughout the atria, more atrial remodeling) and the effect of ablation is considerably poorer. Roughly 50% of cases with persistent atrial fibrillation are cured with ablation therapy. Lung vein isolation is part of the treatment and aims to create a scar around the lung veins so they become electrically isolated from the atrium.
Ablation therapy should be considered in all patients with symptomatic atrial fibrillation which is paroxysmal or persistent. The patient should have tried at least one anti-arrhythmic drug before ablation therapy.
Although ablation therapy is a proven effective method, there is always a risk of future relapse.
Anticoagulation as prophylaxis against thromboembolism
Stroke, transient ischemic attach and peripheral emboli are common in atrial fibrillation and must be addressed. The risk of thromboembolism is not, as previously believed, equal in all forms of atrial fibrillation. A recent meta-analysis by Ganesan et al. showed that paroxysmal atrial fibrillation is associated with a lower risk of stroke than persistent atrial fibrillation. However, the benefits of anticoagulation are equal in the two groups and both should be managed using the same treatment algorithms. Thus, current guidelines on anticoagulation in atrial fibrillation do not put forward any specific advice in relation to the type of atrial fibrillation.
Begin by judging the risk of thromboembolism by using CHADS score and/or CHADS-VA score. The risk of bleeding should be assessed using HAS-BLED score. Patients with a greater risk for thromboembolism than bleeding should be offered anticoagulation. The risk of stroke will be reduced by 70% using cheap anticoagulants such as warfarin. Newer options (dabigatran, apixaban, rivaroxaban) are more expensive, equally effective in reducing stroke events, do not require monitoring of PK/INR, and appear to cause fewer serious bleedings.

