Acute bradycardia with hemodynamic effects is a potentially life-threatening condition and should be managed urgently. The risk of cardiogenic shock and cardiac arrest is high and pharmacological interventions are frequently futile. It is often necessary to establish a transcutaneous pacemaker, which is the only treatment with class I recommendation according to European (ESC) and North American (AHA, ACC) guidelines. As in all clinical emergencies, the airway, breathing, circulation, disability, exposure (ABCDE) approach is applicable in bradycardia (Figure 1). Cardiac output and blood pressure, rather than ECG, are the strongest predictors of adverse outcomes.
Non-acute or asymptomatic bradycardia
Non-acute bradycardia is a common finding in both healthy and diseased individuals. Asymptomatic bradycardia may lack prognostic significance or be physiological, particularly in athletes and young individuals. The severity of symptoms and presence of high-risk arrhythmias on ECG guides the management of non-acute or asymptomatic bradyarrhythmia.
In patients presenting with intermittent symptoms of bradycardia, it is fundamental to establish a temporal correlation between the symptoms and ECG recordings confirming a bradyarrhythmia. Potentially reversible causes should be pursued (Table 2).
Figure 1. Management of acute bradycardia in the emergency setting.
Table 1. Initial evaluation of bradycardia according to ABCDE.
Symptoms of bradycardia
Bradycardia may be an incidental and asymptomatic finding. The absence of symptoms indicates that the bradycardia is compensated by an increase in stroke volume.
Symptomatic bradycardia may present with chronic or acute symptoms, ranging from chronic fatigue and exercise intolerance to sudden cardiac arrest. The most common acute symptoms are dizziness (pre-syncope), hypotension (chock), syncope, chest pain, heart failure and cardiac arrest.
In cases with intermittent symptoms, it is important to establish a temporal correlation between symptoms and episodes of bradyarrhythmia on ECG recordings.
Normal heart rate and normal variants
Normal resting heart rate is 50 to 95 beats per minute in the afternoon. Nocturnal heart rate is on average 20 beats per minute lower (than the average heart rate in the afternoon) in young individuals, and 14 beats per minute lower in the elderly (Brodsky et al, Kantelip et al). Thus, bradyarrhythmia is very common during sleep (Dickinson et al). Pronounced sinus bradycardia is frequently associated with hypoxic episodes caused by obstructive sleep apnea. The following bradyarrhythmias are considered normal findings during sleep:
Bradycardia in atrial fibrillation (bradycardia–tachycardia syndrome)
Individuals with sick sinus syndrome (sinus node dysfunction) are at high risk of developing atrial fibrillation, and vice versa. The pathophysiological explanation for this may be a general degeneration of the atrial conduction system. Individuals with atrial fibrillation and bradycardia have bradycardia–tachycardia syndrome. Careful management is warranted in patients with bradycardia–tachycardia syndrome since episodes of tachyarrhythmia (atrial fibrillation, atrial flutter) cause overdrive suppression of sinus node automaticity, which may result in prolonged sinus pauses or arrests after termination (spontaneous or by intervention) of the atrial tachyarrhythmia. Dizziness, pre-syncope or syncope in patients with atrial fibrillation is suggestive of bradycardia–tachycardia syndrome.
Approximately 65% of individuals with atrial fibrillation have pauses longer than 3 seconds during daytime. Pauses up to 2.8 seconds during daytime and up to 4 seconds during nighttime are considered normal in atrial fibrillation (Pitcher et al).
Cardiac output and blood pressure during bradycardia
Several factors modify the effect of bradycardia on cardiac output (CO) and mean arterial pressure (MAP). Cardiac output is the product of heart rate (HR) and stroke volume (SV), according to the following formula:
CO = HR • SV
Cardiac output and peripheral resistance (SVR, systemic vascular resistance) affect MAP, according to the following formula:
MAP = CO • SVR
If ventricular function is normal, a higher heart rate will result in increased cardiac output, despite the fact that stroke volumes become smaller as heart rate increases (due to reduced diastolic filling time). At very high heart rates (>160 beats/minute), however, the stroke volume will diminish due to the reduced filling time (Table 2).
Situation
Heart rate
Stroke volume
Cardiac output
Comment
Mild tachycardia
100-160 bpm
↓
↑
CO increases because increased HR dominates over decreased SV.
Pronounced tachycardia
>160 bpm
↓↓↓
↓
CO decreases because decreasing SV dominates over increased HR.
Mild bradycardia
40–50 bpm
↑
↓
CO decreases because increased SV does not compensate for decreased HR.
Pronounced bradycardia
<40 bpm
↑
↓↓↓
CO decreases substantially because increased SV does not compensate for decreased HR.
Table 2. The effect of heart rate and stroke volume on cardiac output. Abbreviations: bpm = beats per minute.
A halving of the heart rate (i.e bradycardia) has a significantly greater effect on cardiac, as compared with a doubling of the heart rate (tachycardia). This is explained by the fact that the heart has a very limited capacity to increase stroke volume (i.e the capacity to increase stroke volume is insufficient to compensate for severe bradycardia).
The cardiac conduction system
The cardiac conduction system is discussed in the chapter Cardiac Electrophysiology. Aspects relevant to bradycardia are discussed here. The arterial blood supply to the conduction system is presented in Figure 2. The electrical impulse that initiates the cardiac cycle originates in the sinoatrial node (sinus node), which is located in the sulcus terminalis. These cells possess automaticity, which is the ability to depolarize spontaneously. The sinus node depolarization spreads throug the atria to the atrioventricular (AV) node, which transmits the impulse to the ventricular myocardium via His bundle, the right bundle branch and left bundle branch. His bundle travels from the AV node to the muscular septum via the membraneous septum. His bundle divides into a smaller anterior fascicle and larger posterior fascicle. The sinoatrial node is supplied with blood by the sinus node artery, which originates from the RCA (right coronary artery) in 80% and LCx (left circumflex artery) in 20%. The AV node is supplied with blood by the atrioventricular nodal artery, which originates from the proxial PDA (posterior descending artery). The PDA is a branch of the RCA in 85% of cases and LCx in 15% of cases.
The intrinsic rate of depolarization in the sinoatrial node is 85 to 105 beats pre minute (Jose et al). Resting heart rate in healthy individuals is lower due to parasympathetic dominance during rest. The conduction system is innervated by sympathetic and parasympathetic fibers (Vagus nerve). These fibers modulate the rate of depolarization and impulse transmission through all components of the conduction system. Sympathetic activity increases the rate of depolarization and impulse transmission. Parasympathetic activity slows rate of depolarization and impulse transmission. Strong parasympathetic stimulation can temporarily depress automaticity in the sinoatrial node and cause brief arrest, or block transmission through the AV node and cause transient AV block.
Figure 2. Arterial blood supply to the conduction system.
Blood pressure in bradycardia
Blood pressure is a strong predictor of cardiogenic shock and cardiac arrest. Bradycardia with hypotension is a critical condition that requires immediate treatment to prevent circulatory collapse.
During bradycardia, however, the blood pressure may be normal or high as a result of sympathetic activation. This is explained by the fact that bradycardia leads to the release of catecholamines (adrenaline [epinephrine] and noradrenaline [norepinephrine]) which induce vasoconstriction. Hence, blood pressure may be normal during bradycardia despite severely reduced cardiac output.
Hypertension is a sign of critical bradycardia with pronounced sympathetic activation. In such cases, the blood pressure must not be lowered, since it may cause cardiogenic shock. Blood pressure normalizes when the heart rate and cardiac output are normalized.
• Cardiac output is always low during pronounced bradycardia. • Normal blood pressure does not rule out critical bradycardia. • High blood pressure should not be lowered during bradycardia.
Torsade de pointes during bradycardia
Bradycardia can prolong the QT interval and subsequently increase the risk of torsade de pointes (TdP). Bradycardia is a significant risk factor for torsade de pointes (Choo et al). Risk factors for torsade de pointes in bradycardia are as follows (Topilski et al):
First-degree AV block does not cause bradycardia but may occur intermittently in second-degree AV block, third-degree AV block and sinus node dysfunction.
Pronounced first-degree AV-block (PR interval >350 ms) may disrupt AV synchrony, which may affect cardiac output.
Mobitz type 1 second-degree AV block
Mobitz type 1 may be physiological in young individuals and athletes, in which case it is asymptomatic and caused by increased vagal tone.
Among cases with pathological Mobitz type 1 blocks, 75% are located in the AV node (typically with normal QRS duration, i.e <120 ms). The remaining 25% are infranodal blocks (i.e located in His bundle, the bundle branches, or fascicles).
The escape rhythm in Mobitz type 1 is usually stable and hypotension is uncommon.
Mobitz type 2 second-degree AV block
Mobitz type 2 is always pathological.
Location: <5% in AV node, 20% in His bundle; 75% in the bundle branches.
The arrhythmia is mostly symptomatic, with a high risk of progression to complete AV block.
The escape rhythm is mostly ventricular and therefore hemodynamically insufficient and unreliable.
AV block 3 (complete AV block, AV dissociation)
Third-degree AV-blocks are mostly infranodal.
The escape rhythm can originate in the AV system (His-Purkinje fibers) or the ventricular myocardium.
Escape rhythm generated proximally to the bifurcation of His bundle produces narrow QRS complexes (<120 ms), heart rate >40/min, moderate symptoms, and typically a reliable escape rhythm.
Escape rhythm generated distally to the bifurcation produces wide QRS complexes, slow rhythm and unreliable escape rhythm. The symptoms are more pronounced (pre-syncope, syncope, heart failure, hypotension).
Frequent ventricular extrasystoles that fail to generate stroke volumes. The effective (i.e pulse generating) ventricular rate may be very low during frequent ventricular extrasystoles.
Frequent supraventricular extrasystoles that fail to generate stroke volumes. As with ventricular extrasystoles, the effective (i.e pulse generating) ventricular rate may be very low during frequent supraventricular extrasystoles.
Ventricular and supraventricular extrasystoles are uncommon causes of bradycardia. In these cases, bradycardia can only be detected by palpating the pulse.
Causes of AV block
50% of all AV blocks are caused by degeneration/fibrosis of the cardiac conduction system.
The majority are caused by degeneration/fibrosis in the sinus node and atrial conduction fibers. This degeneration can also involve the ventricular conduction system.
A minority is caused by etiologies listed in Table 3.
Inferior myocardial ischemia/infarction (infarct-related bradycardia is usually transient, not requiring pacemaker) Anterior myocardial ischemia/infarction (infarct-related bradycardia is usually permanent, requiring pacemaker
Increased vagal tone Increased intracranial pressure (ICP)
Yes
Table 3. Causes of bradycardia. 1BRASH: Bradycardia Renal failure AV block and Shock : BRASH affects patients with hyperkalemia who are using AV-blocking medications. These patients may experience life-threatening bradycardia due to the synergistic effect between hyperkalemia and AV-blocking medications (eg beta-blockers, calcium channel blockers).
Nodal vs. infranodal obstruction
Nodal blocks are defined as blocks located in the AV node. Infranodal blocks are located in the bundle of His, the bundle branches, the fascicles or at multiple levels below the AV node. The prognosis is substantially worse in infranodal blocks, which typically require a permanent pacemaker, unless a reversible cause is identified. Third-degree AV-blocks are typically infranodal. The escape rhythm will typically indicate the location of the block. Escape rhythm with a narrow QRS complex and ventricular rate between 40 to 60 beats per minute suggests a nodal block. Wide QRS and ventricular rate slower than 40 beats per minute suggests an infranodal block.
Features
Nodal block
Infranodal block
QRS duration
Typically narrow (<120 ms)
Typically wide (>120 ms)
PR interval
Typically prolonged
Typically not affected
Escape rhythm
40–60 bpm
<40 bpm
Wenchebach periods
Often seen
Rarely seen
Effect of atropine
Increased AV conduction
Mostly no effect
Effect of catecholamines (isoprenaline)
Increased AV conduction
May accelerate escape rhythm
Effect of exercise
None or enhanced AV conduction
None or worsened AV conduction
Prognosis (escape rhythm)
Better (stable escape rhythm)
Worse (unstable escape rhythm)
Table 4. Differentiation of nodal vs. infranodal blocks. Note that intra-Hisian blocks (i.e. blocks in the bundle of His) may exhibit narrow QRS complexes.
In the event of manifest or impending circulatory collapse, transcutaneous pacing must be started immediately. The risk of circulatory collapse is highest with AV block 2 Mobitz type 2 and AV block 3. The only treatment with a class I recommendation for the management of acute bradycardia is transcutaneous pacing. Pharmacological interventions (Table 4) should be considered temporary, often insufficient, treatments that can be attempted until a pacemaker is established.
Drug
Effect
Dose, kinetics
Comment
Atropine
Acetylcholine receptor antagonist
1 mg IV every 3-5 minutes, maximum 3 mg IV.
T½ 3 h. 50% renal elimination.
• Typically the first choice of drug. • Effective in sinus bradycardia or AV node block. • Dose <0.5 mg may worsen bradycardia and should not be given. • Relative contraindications are ileus, glaucoma.
Isoprenaline / Isoproterenol
α-1, α-2, β-1, β-2 agonist
Start infusion at 4 μg/min and titrate to desired result
T½ 1 min
• May cause ventricular arrhythmias (dose-dependent). • Prolonged use often causes headaches, tremors. • Effective if bradycardia is caused by beta blockers.
Adrenaline (Epinephrine)
α and β agonist
Infusion of 2–10 μg/min (titrate as needed).
T½ 5 min.
• Effective if hypotension is present. • Can be given as a bolus. • Effective if bradycardia is caused by beta blockers.
Dopamine
Dopamine receptor agonist, α- and β-agonist
Infusion of 5−20 μg/kg/min
T½ 2 min
• Avoid boluses. • Effective if bradycardia is caused by beta blockers.
Dobutamine
β-1 agonist
Infusion of 3−10 μg/kg/min.
T½ 2 min
Effective if inotropic effect is required.
Theophylline / theophyllamine / aminophylline
Adenosine receptor antagonist, phosphodiesterase inhibitor. Exact mechanism is unknown.
100−200 mg slow iv injection.
Rarely used.
Glucagon
Counteracts beta blockers. An antidote to beta blockers.
2–10 mg bolus followed by 2–5 mg/h infusion
Antidote to beta blockers.
Calcium
Counteracts calcium channel blockers (CCB). Antidote to CCBs.
10 ml calcium 0.2 mmol/ml iv.
Antidote to CCBs.
Digoxin antibodies
Binds to digoxin.
Digitalis antidote (anti-digoxin, Fab fragment).
Given in case of suspected digoxin intoxication.
Table 4. Pharmacological treatment of acute bradycardia.
Atropine
Evidence: Class IIa recommendation
Atropine is the first choice for the pharmacological treatment of acute bradycardia.
Dosage: 1 mg iv, every 3-5 minutes, to a maximum of 3 mg.
Doses lower than 0.5 mg IV may worsen bradycardia and should never be given.
The effect of atropine is temporary.
If atropine is ineffective, isoprenaline, adrenaline (epinephrine) or dopamine can be tried.
Atropine counteracts acetylcholine-mediated bradycardia by inhibiting the effect of acetylcholine on the sinus node and AV node. Atropine is effective in sinus bradycardia and AV block located in the AV node.
Atropine is typically ineffective in complete AV block and Mobitz type 2 second-degree AV block.
Atropine is not used in patients with heart transplantation.
Isoprenaline (isoproterenol)
Evidence: Class IIa recommendation
Isoprenaline is a second-line pharmacological treatment for acute bradycardia.
Dosage: Start infusion at 4 μg/min and titrate to the desired result.
Half-life: 5 minutes.
Isoprenaline enhances AV conduction in nodal blocks. In infranodal blocks, isoprenaline is effective only if it induces an escape rhythm, or enhances the automaticity of an existing escape rhythm..
Adrenaline (epinephrine)
Evidence: Class IIb recommendation
Effective in hypotension and when an inotropic effect is required.
Dosage: Infusion of 2–10 μg/min (titrate as needed).
Can be added to dopamine.
Dopamine
Evidence: Class IIb recommendation
Effective in hypotension and when an inotropic effect is required.
Dosage: Infusion 5−20 μg/kg/min.
Can be added to adrenaline.
Temporary pacemaker
Transcutaneous pacemaker
Evidence: Class I recommendation
Most defibrillators have a pacemaker function, allowing the device to operate as an external pacemaker. (Video 1, Figure 2, Figure 3).
A pacemaker is the safest treatment for acute bradycardia.
A transcutaneous pacemaker should be established immediately if there is a risk of hemodynamic collapse.
AV block 2 Mobitz type 2 and AV block 3 are strong indications for a transcutaneous pacemaker.
Figure 2. Example showing Zoll R Series defibrillator. Note that the Mode Selector is set to Pacer to activate the pacemaker settings.
Video 1. Example of transcutaneous pacemaker with Zoll R Series . The function looks similar for other manufacturers.
Pain and discomfort during transcutaneous pacing
Although transcutaneous pacing can be unpleasant or somewhat painful, all patients tolerate the procedure. Pain is caused by muscle contractions. Administration of sedatives (midazolam) or analgesics (morphine) is recommended, using the following doses:
Midazolam : 1–3 mg initial dose. Total dose 4-8 mg. Lower dose range in cases aged >60 years.
Morphine : 2.5 mg IV.
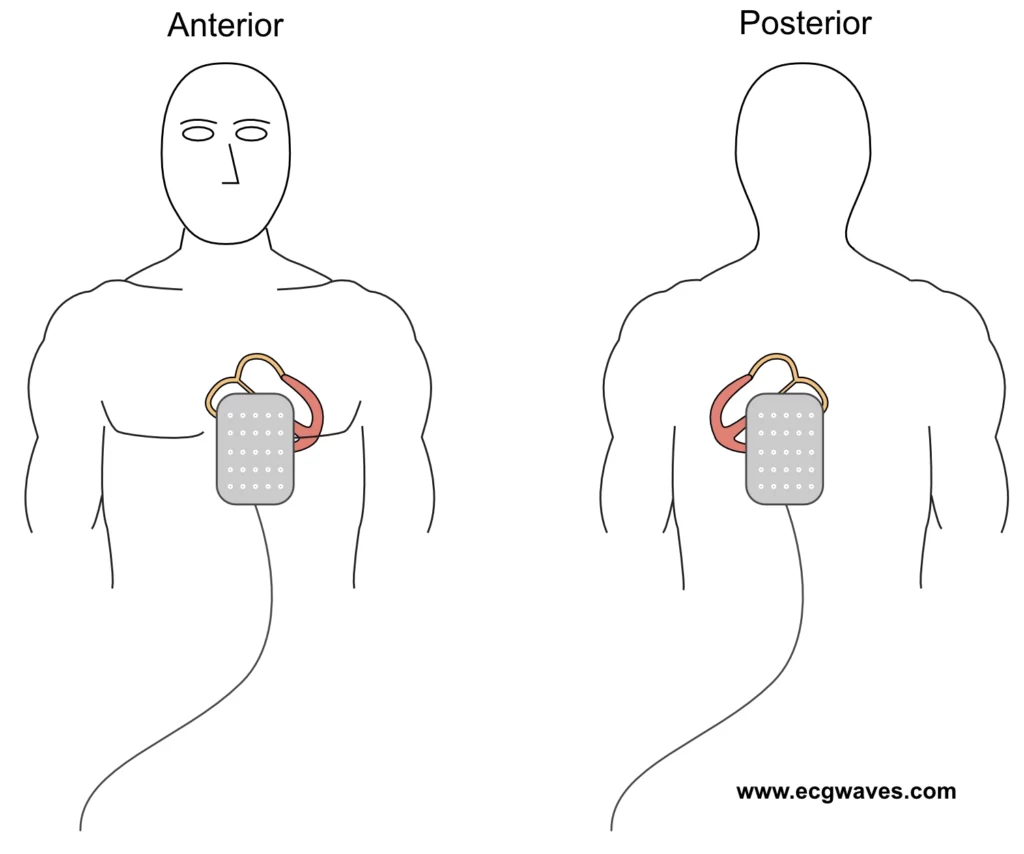
Figure 4. Placement of electrode pads in the anteroposterior direction for transcutaneous pacing.
How to perform transcutaneous pacing
Explain to the patient the purpose of the procedure.
Administer sedatives / analgesics.
Position electrode pads in anteroposterior direction (Figure 4).
If there is time, trim chest/back hair (do not shave). Dry the skin if wet.
Do not relocate already attached pads (the adhesive becomes poor).
Activate the pacemaker function (Video 1, Figure 2, Figure 3).
Set the pacing rate to 50 beats/min.
Gradually increase the current (start with 20 mA) .
Identify the pacemaker spikes (stimulation artifacts) on the ECG recording.
Determine if pacemaker spikes are followed by QRS complexes (indicating electrical capture).
If electrical capture is visible, palpate the femoral artery to examine whether there is mechanical capture (i.e ventricular contractions).
Monitor blood pressure and pulse oximetry.
When the threshold for capture (lowest current producing mechanical capture) is identified, the output (current) is increased by 10% (in order to provide stimulations with a safety margin).
Most patients require a current in the range of 20 to 140 mA
Avoid unnecessary pacing by using a low base frequency (e.g. 30–40 beats/min).
How to perform transcutaneous pacing during asystole
Follow the same procedure as above but start with maximum current strength (output) and gradually reduce the current until stimulation fails to produce capture. Then increase the current until capture is obtained, and another 10% output as a safety margin.
Checking transcutaneous pacing
Mechanical capture is confirmed by palpating a peripheral pulse (femoral artery) or assessing pulse oximetry. Avoid evaluating the pulse in the carotid artery (pectoral muscle contractions may be mistaken as arterial pulsations).
Muscle contractions are not equivalent to mechanical capture.
If the pacemaker stimulates more than necessary, there is undersensing, which means that the pacemaker does not detect the ventricular complexes (and therefore continues to pace). This is resolved by relocating the ECG leads so that they detect larger QRS amplitudes or increasing the gain on the defibrillator.
If the pacemaker does not stimulate due to artifacts there is oversensing, which can be resolved by eliminating the artifacts or relocating the leads.
Transvenous pacing
A transvenous pacemaker should be established if transcutaneous pacing is ineffective.
Transvenous pacemaker requires higher competence to establish and also entails a risk of infection, perforation and tamponade.
Access can be obtained via the jugular vein or the femoral vein. The introduction of a pacemaker lead via the jugular vein carries a risk of local thrombosis or infection, which complicates later pacemaker implantation. Pacing via the femoral vein requires immobilization of the patient since movements can cause dislocation of the lead.
A transvenous pacemaker can use a screw electrode, which can remain for up to 6 weeks and carries a significantly lower risk of lead dislocation.
Steinbach M, Douchet MP, Bakouboula B, Bronner F, Chauvin M. Outcome of patients aged over 75 years who received a pacemaker to treat sinus node dysfunction. Arch Cardiovasc Dis 2011;104:89 –96.
Li H, Lakkireddy D, Korlakunta H, Rovang K, Hee T. Pacemaker utilization during permanent atrial fibrillation in patients who received pacemaker implantation for sinus node dysfunction. Am J Cardiol 2005;96:942–945.
Andersen HR, Nielsen JC, Thomsen PE, et al. Long-term follow-up of patients from a randomized trial of atrial versus ventricular pacing for sick-sinus syndrome. Lancet 1997;350:1210-1216
Ferrer MI. The sick sinus syndrome in atrial disease. JAMA 1968;206:645– 652.
Van Gelder IC, Groenveld HF, Crijns HJ, Tuininga YS, Tijssen JG, Alings AM, Hillege HL, Bergsma-Kadijk JA, Cornel JH, Kamp O, Tukkie R, Bosker HA, Van Veldhuisen DJ, Van den Berg MP; RACE II Investigators. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med 2010;362:1363–1373.