Sinoatrial block (SA block): ECG criteria, causes and clinical features
Sinoatrial block (SA block): from ECG to clinical management
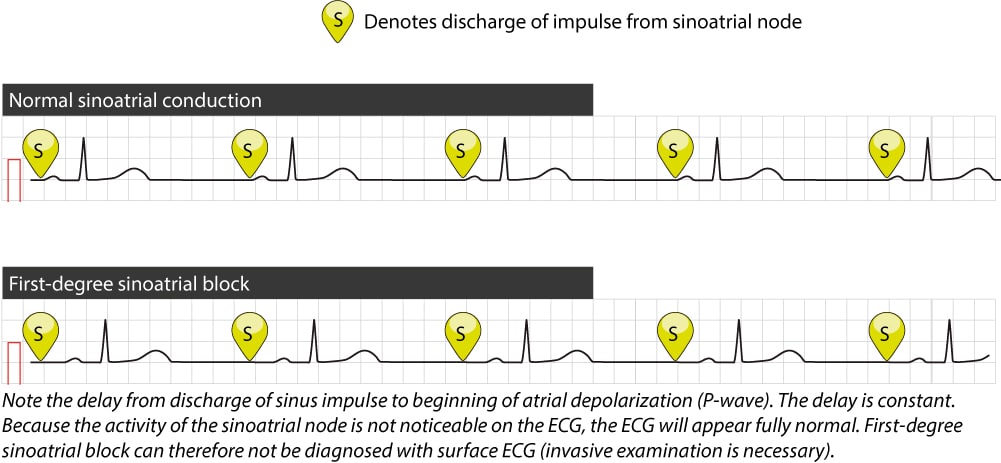
Sinoatrial (SA) block implies that the impulses discharged in the sinoatrial node are either not conducted to the atria or are so with a delay. This manifests with loss of P-waves (loss of atrial activation) and consequently loss of QRS complexes (loss of ventricular depolarization).
Sinoatrial blocks are subdivided into three degrees according to the nature of the block. The nature of these blocks is very similar to the atrioventricular (AV) blocks. Importantly, first-degree sinoatrial block and third-degree sinoatrial block cannot be diagnosed using surface ECG (i.e. ECG recorded on the body surface). This is because the electrical potentials generated by the sinoatrial node are much too small to be detected on the surface ECG. Intracardiac electrodes – with the placement of electrodes against the sinoatrial node – are necessary to diagnose first- and third-degree sinoatrial block. However, a second-degree sinoatrial block may be diagnosed using conventional ECG.
Causes of sinoatrial (SA) block
The following conditions cause sinoatrial block:
- Sinus node dysfunction (SND)
- Perimyocarditis
- Acute myocardial infarction (or ischemia)
- Drug side effects (procainamide, digitalis)
- Well-trained athletes display sinoatrial block as a physiological and normal finding.
First-degree sinoatrial (SA) block
First-degree sinoatrial block implies that the time interval from the discharge of the impulse in the sinoatrial node to the onset of atrial depolarization is prolonged. As seen in Figure 1 this merely entails that the distance between the sinus impulse and P-wave is increased and this cannot be discerned from the surface ECG (because discharge of the impulse in the sinoatrial node is not noticeable on surface ECG).
Second-degree sinoatrial (SA) block
Second-degree sinoatrial block is further subdivided into type 1 and type 2. The block, in both types, may be regular, temporary, or intermittent.
Second-degree sinoatrial (SA) block type 1 (Wenckebach block)
In type 1 second-degree sinoatrial block there is a delay in the conduction from the sinoatrial node to the atrium and this delay increases gradually until one impulse is completely blocked and a loss of P-wave occurs. The P-P interval is gradually decreased. The ensuing pause is twice as long as the cardiac cycle preceding the block. The P-P interval after the pause is longer than the P-P interval before the pause. Refer to Figure 2 (below). This type of block, where there is a gradual exhausting of the conduction before it is completely blocked, is referred to as Wenckebach phenomenon (also referred to as Wenckebach periodicity).
Log in to view image, video, quiz, text

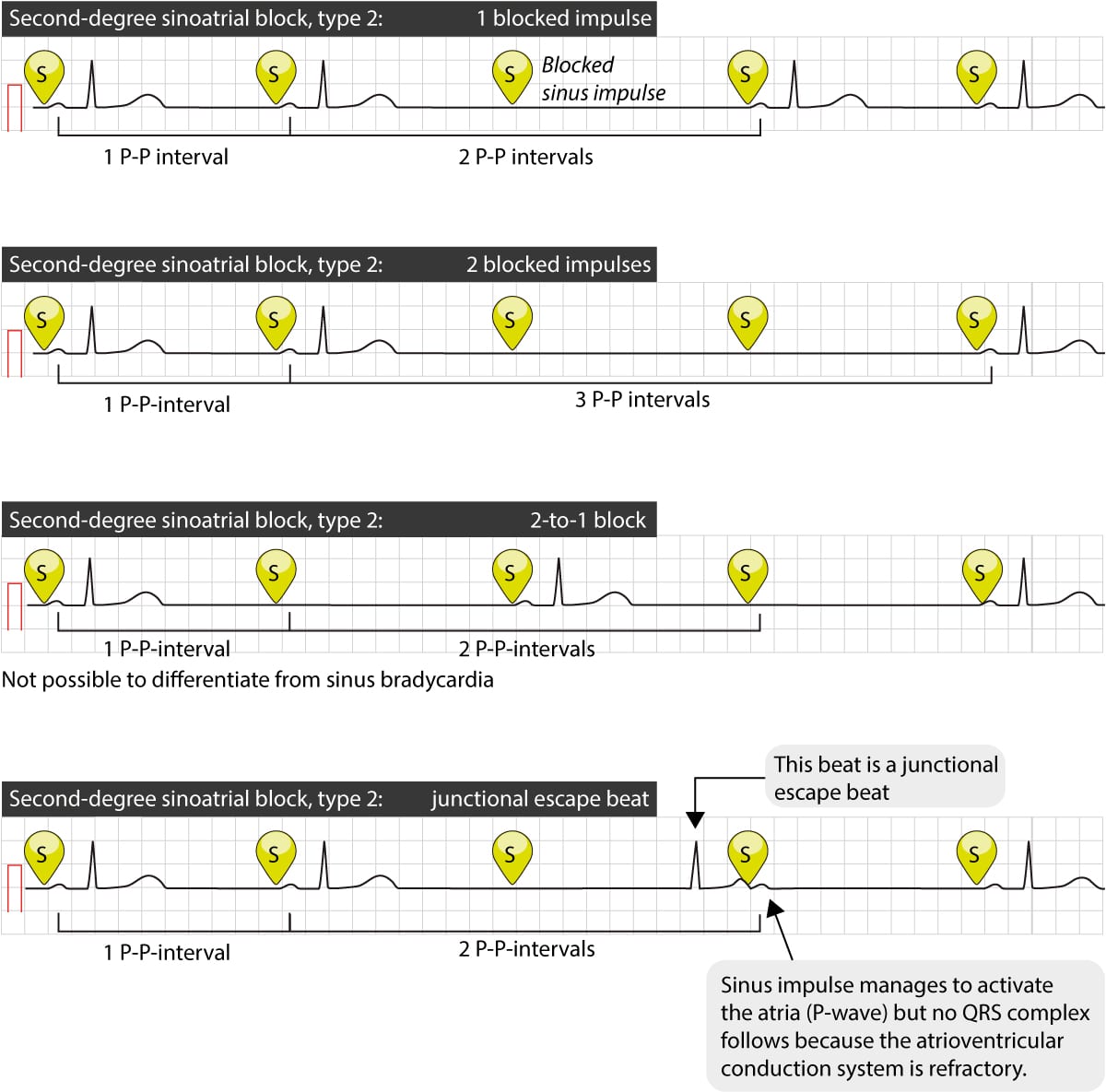
Second-degree sinoatrial (SA) block type 2
In type 2 second-degree sinoatrial block impulses are blocked sporadically (without any Wenckebach phenomenon). The pauses between the visible beats are always multiples of the normal P-P interval (Figure 3). Typically, there will be 2 to 4 P-P intervals between the beats (implying that one, two or three sinus impulses are blocked). This is illustrated in Figure 3 (below).
Third-degree sinoatrial (SA) block
Third-degree sinoatrial block implies that no impulses are conducted from the sinoatrial node to the atrium. Hence, the maintenance of cardiac rhythm (and thus life) will depend on the awakening of a latent pacemaker. Studies clearly show that a latent pacemaker will virtually always awake, such that the mortality in third-degree sinoatrial block is very low. The salvaging rhythm is referred to as an escape rhythm and it is likely to arise in the atrial myocardium (specific clusters of myocardium with automaticity), the junctional area (near the atrioventricular node), or in the His-Purkinje network (in that order). Refer to Figure 4. However, third-degree sinoatrial block cannot be discerned from surface ECG.
Log in to view image, video, quiz, text
Management and treatment of sinoatrial (SA) block
Sinoatrial blocks may cause bradycardia. Evidence shows that the bradycardia and the sinoatrial block itself do not convey any significant increase in mortality. However, a sinoatrial block may compromise cardiac output and cause symptoms or worsen symptoms. Symptomatic sinoatrial block is therefore frequently treated with a permanent pacemaker. Treatment alternatives are discussed in the article on sinus node dysfunction.

