Clinical ECG Interpretation
-
Introduction to ECG Interpretation6 Chapters
-
Cardiac electrophysiology and ECG interpretation
-
Cardiac electrophysiology: Action potential, automaticity and vectors
-
The ECG leads: Electrodes, limb leads, chest (precordial) leads and the 12-Lead ECG
-
The Cabrera format of the 12-lead ECG and inverted lead aVR
-
ECG interpretation: Characteristics of the normal ECG (P-wave, QRS complex, ST segment, T-wave)
-
How to interpret the ECG: A systematic approach
-
Cardiac electrophysiology and ECG interpretation
-
Arrhythmias and arrhythmology24 Chapters
-
Mechanisms of cardiac arrhythmias: from automaticity to re-entry (reentry)
-
Aberrant ventricular conduction (aberrancy, aberration)
-
Premature ventricular contractions (premature ventricular complex, premature ventricular beats)
-
Premature atrial contraction (premature atrial beat / complex): ECG and clinical implications
-
Sinus rhythm: physiology, ECG criteria & clinical implications
-
Sinus arrhythmia (respiratory sinus arrhythmia)
-
Sinus bradycardia: definitions, ECG, causes and management
-
Chronotropic incompetence (inability to increase heart rate)
-
Sinoatrial arrest & sinoatrial pause (sinus pause / arrest)
-
Sinoatrial block (SA block): ECG criteria, causes and clinical features
-
Sinus node dysfunction (SND) and sick sinus syndrome (SSS)
-
Sinus tachycardia & Inappropriate sinus tachycardia
-
Atrial fibrillation: ECG, classification, causes, risk factors & management
-
Atrial flutter: classification, causes, ECG criteria and management
-
Ectopic atrial rhythm (EAT), atrial tachycardia (AT) & multifocal atrial tachycardia (MAT)
-
Atrioventricular nodal reentry tachycardia (AVNRT): ECG features & management
-
Pre-excitation, Atrioventricular Reentrant (Reentry) Tachycardia (AVRT), Wolff-Parkinson-White (WPW) syndrome
-
Junctional rhythm (escape rhythm) and junctional tachycardia
-
Ventricular rhythm and accelerated ventricular rhythm (idioventricular rhythm)
-
Ventricular tachycardia (VT): ECG criteria, causes, classification, treatment
-
Long QT (QTc) interval, long QT syndrome (LQTS) & torsades de pointes
-
Ventricular fibrillation, pulseless electrical activity and sudden cardiac arrest
-
Pacemaker-mediated tachycardia (PMT): ECG and management
-
Diagnosis and management of supraventricular and ventricular tachyarrhythmias: Narrow complex tachycardia & wide complex tachycardia
-
Mechanisms of cardiac arrhythmias: from automaticity to re-entry (reentry)
-
Myocardial Ischemia & Infarction24 Chapters
-
Introduction to Coronary Artery Disease (Ischemic Heart Disease)
-
Classification of Acute Coronary Syndromes (ACS) & Acute Myocardial Infarction (AMI)
-
A New Approach to Acute Coronary Syndromes: Occlusion MI (OMI) vs. Non-Occlusion MI (NOMI)
-
Clinical application of ECG in chest pain & acute myocardial infarction
-
Diagnostic Criteria for Acute Myocardial Infarction: Cardiac troponins, ECG & Symptoms
-
Cardiac troponin I (TnI) and T (TnT): Interpretation and evaluation in acute coronary syndromes
-
Myocardial Ischemia & infarction: Cellular changes, ECG and symptoms
-
The left ventricle in myocardial ischemia and infarction
-
Factors that modify the natural course in acute myocardial infarction (AMI)
-
ECG in myocardial ischemia: ischemic changes in the ST segment & T-wave
-
ST segment depression in myocardial ischemia and differential diagnoses
-
ST segment elevation in acute myocardial ischemia and differential diagnoses
-
ST elevation myocardial infarction (STEMI) without ST elevations on 12-lead ECG
-
T-waves in ischemia: hyperacute, inverted (negative), Wellen's sign & de Winter's sign
-
ECG manifestations of left main coronary artery (LMCA) occlusion and critical stenosis
-
ECG signs of myocardial infarction: pathological Q-waves & pathological R-waves
-
Other ECG changes in ischemia and infarction
-
Supraventricular and intraventricular conduction defects in myocardial ischemia and infarction
-
ECG localization of myocardial infarction / ischemia and coronary artery occlusion (culprit)
-
The ECG in assessment of myocardial reperfusion
-
Approach to patients with chest pain: differential diagnoses, management & ECG
-
Stable Coronary Artery Disease (Angina Pectoris): Diagnosis, Evaluation, Management
-
NSTEMI (Non-ST Elevation Myocardial Infarction) & Unstable Angina: Diagnosis, Criteria, ECG, Management
-
STEMI (ST Elevation Myocardial Infarction): Diagnosis, ECG, Criteria, and Management
-
Introduction to Coronary Artery Disease (Ischemic Heart Disease)
-
Conduction Defects11 Chapters
-
Overview of atrioventricular (AV) blocks
-
First-degree AV block (AV block I, AV block 1)
-
Second-degree AV block: Mobitz type 1 (Wenckebach) & Mobitz type 2 block
-
Third-degree AV block (3rd degree AV block, AV block 3, AV block III)
-
Management and treatment of AV block (atrioventricular blocks)
-
Intraventricular conduction delay: bundle branch blocks & fascicular blocks
-
Right bundle branch block (RBBB): ECG, criteria, definitions, causes & treatment
-
Left bundle branch block (LBBB): ECG criteria, causes, management
-
Left bundle branch block (LBBB) in acute myocardial infarction: the Sgarbossa criteria
-
Fascicular block (hemiblock): Left anterior & left posterior fascicular block
-
Nonspecific intraventricular conduction delay (defect)
-
Overview of atrioventricular (AV) blocks
-
Cardiac Hypertrophy & Enlargement5 Chapters
-
Atrial and ventricular enlargement: hypertrophy and dilatation on ECG
-
ECG in left ventricular hypertrophy (LVH): criteria and implications
-
Right ventricular hypertrophy (RVH): ECG criteria & clinical characteristics
-
Biventricular hypertrophy ECG and clinical characteristics
-
Left atrial enlargement (P mitrale) & right atrial enlargement (P pulmonale) on ECG
-
Atrial and ventricular enlargement: hypertrophy and dilatation on ECG
-
Drugs & Electrolyte Imbalance3 Chapters
-
Genetics, Syndromes & Miscellaneous7 Chapters
-
ECG J wave syndromes: hypothermia, early repolarization, hypercalcemia & Brugada syndrome
-
Brugada syndrome: ECG, clinical features and management
-
Early repolarization pattern on ECG (early repolarization syndrome)
-
Takotsubo cardiomyopathy (broken heart syndrome, stress induced cardiomyopathy)
-
Pericarditis, myocarditis & perimyocarditis: ECG, criteria & treatment
-
Eletrical alternans: the ECG in pericardial effusion & cardiac tamponade
-
Long QT Syndrome (LQTS)
-
ECG J wave syndromes: hypothermia, early repolarization, hypercalcemia & Brugada syndrome
-
Exercise Stress Testing (Exercise ECG)6 Chapters
-
Introduction to exercise stress testing (treadmill test, exercise ECG)
-
Indications, Contraindications, and Preparations for Exercise Stress Testing
-
Exercise stress test (exercise ECG): protocols, evaluation & termination
-
Exercise stress testing in special patient populations
-
Exercise physiology: from normal response to myocardial ischemia & chest pain
-
Evaluation of exercise stress test: ECG, symptoms, blood pressure, heart rate, performance
-
Introduction to exercise stress testing (treadmill test, exercise ECG)
ECG J wave syndromes: hypothermia, early repolarization, hypercalcemia & Brugada syndrome
J-wave syndromes: early repolarization pattern, Brugada syndrome, hypercalcemia and hypothermia
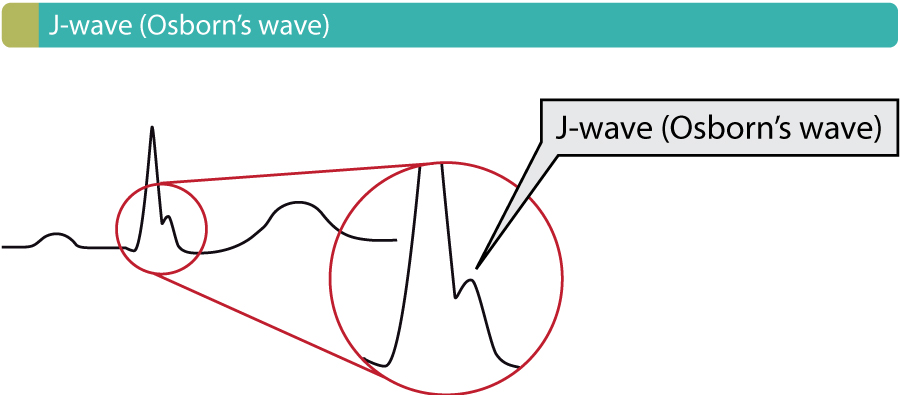
The J wave – also referred to as Osborn’s wave – is defined as a wave occurring at the J point (Figure 1). Conditions in which the J wave occurs may be referred to as J wave syndromes. J waves are typically most pronounced in the anterolateral (V3, V4, V5, V6) and inferior (II, aVF and III) leads. There are four principal causes of J waves, namely hypothermia, Brugada syndrome, early repolarization and hypercalcemia.
Early repolarization, Brugada syndrome and hypercalcemia are discussed separately. Please refer to these articles. ECG examples of each condition are presented below.
The ECG in Brugada syndrome
Brugada syndrome is a rare channelopathy (an electrical disorder caused by mutations in cardiac ion channels) which predisposes the individual to syncope, ventricular arrhythmias (ventricular tachycardia, ventricular fibrillation) and sudden cardiac death. There are three types of ECG manifestations, referred to as type 1, type 2 and type 3 Brugada syndrome. Refer to Figure 2 for ECG example of type 1 Brugada syndrome (note the large J waves in V2–V3).
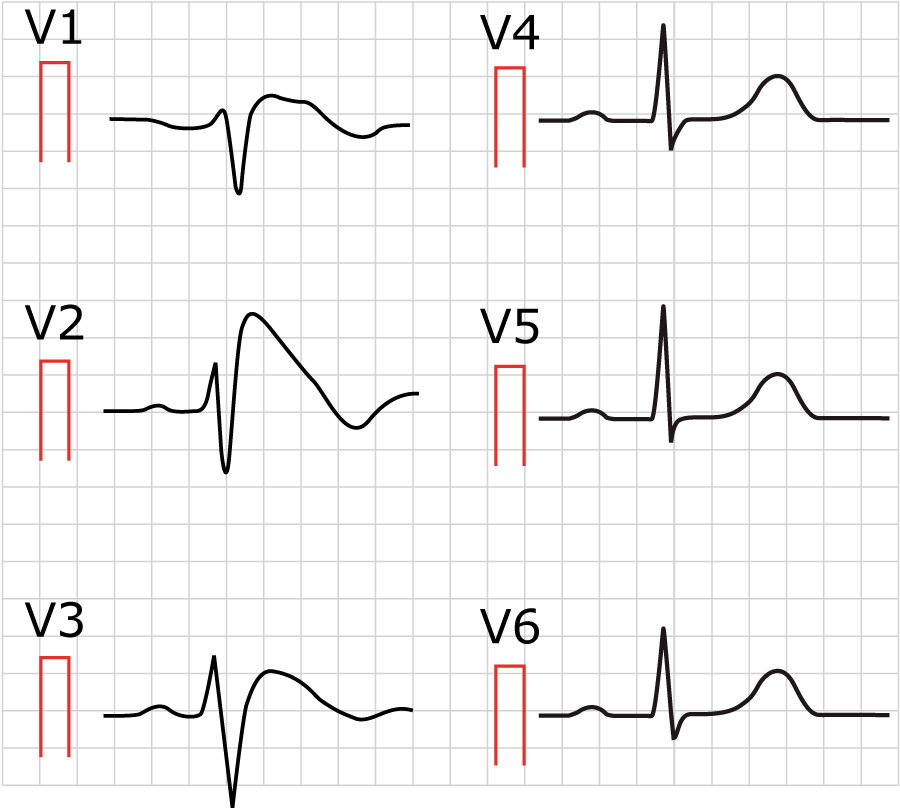
Type 1 Brugada syndrome reminds somewhat of right bundle branch block (RBBB) in leads V1–V3, but the QRS duration is not prolonged in leads V5–V6 (which is not consistent with RBBB, in which there must be wide QRS complexes). In type 1 Brugada syndrome, the ST segment elevation has a coved shape in V1, V2 or V3. The ST segment starts at the apex of the second R-wave and is downsloping. The T-wave is negative (inverted).
Early repolarization pattern
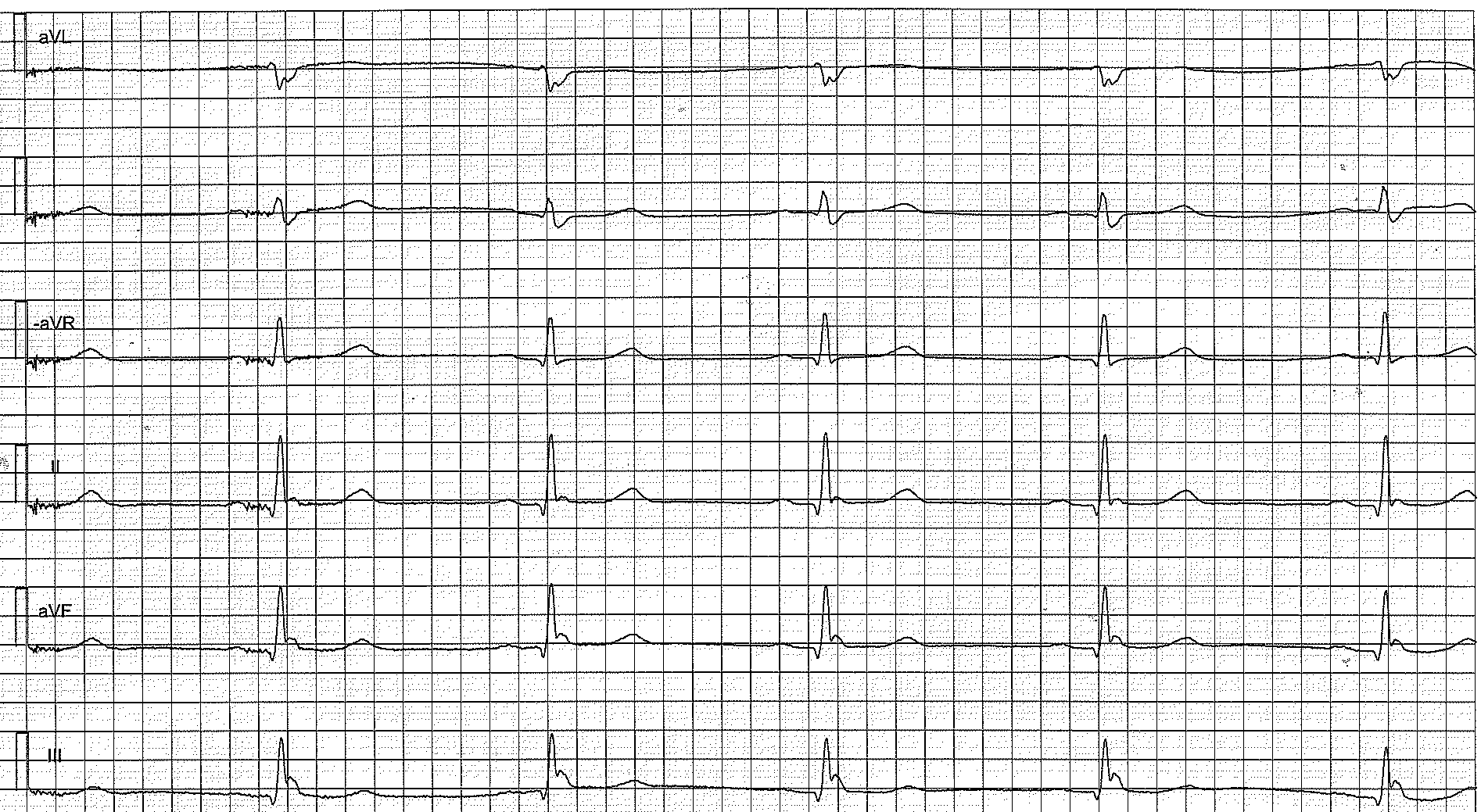
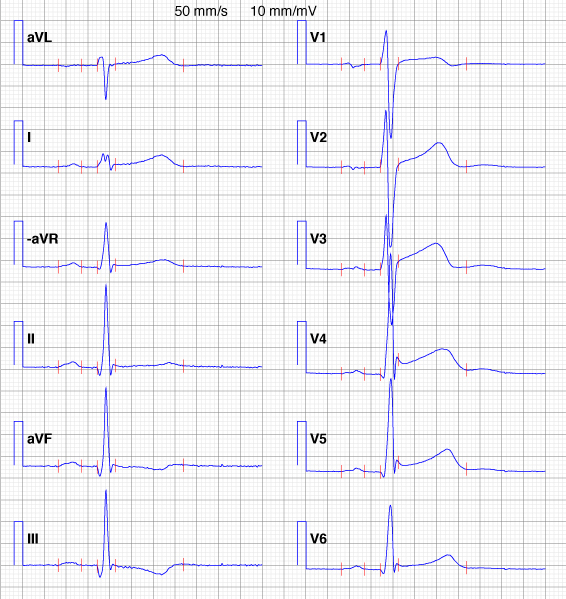
Early repolarization occurs in 5% to 10% of all males. It is less common among women (prevalence 2% to 4%). The condition has been recognized for decades, and it has been regarded as a benign form of ST segment elevation with slurring or notching at the J point. A notch at the J point is actually a J wave.
The term “early repolarization” was used to describe what appeared to be a premature repolarization on the ECG. As seen in Figures 3 and 4, the ST segment elevations are indeed associated with what appears to be an interruption in the QRS complex and initiation of repolarization. However, no study to date has been able to demonstrate that the repolarization is actually early and, moreover, this condition is associated with five times as great a risk of sudden cardiac death. The prefix “benign” must therefore not be used. The risk of sudden cardiac death is greatest if the early repolarization pattern occurs in the inferior limb leads (II, aVF and III).
ECG features of early repolarization
- The ST segment elevations are concave and most pronounced in the chest leads. T-waves have high amplitude.
- The hallmark of early repolarization is the end-QRS slurring or end-QRS notching (the notch is the J wave!).
References
An in-depth discussion regarding J wave syndromes is provided by Charles Antzelevitch. Note that Brugada syndrome and early repolarization are discussed separately here on ecgwaves.com.

