The Cabrera format of the 12-lead ECG and inverted lead aVR
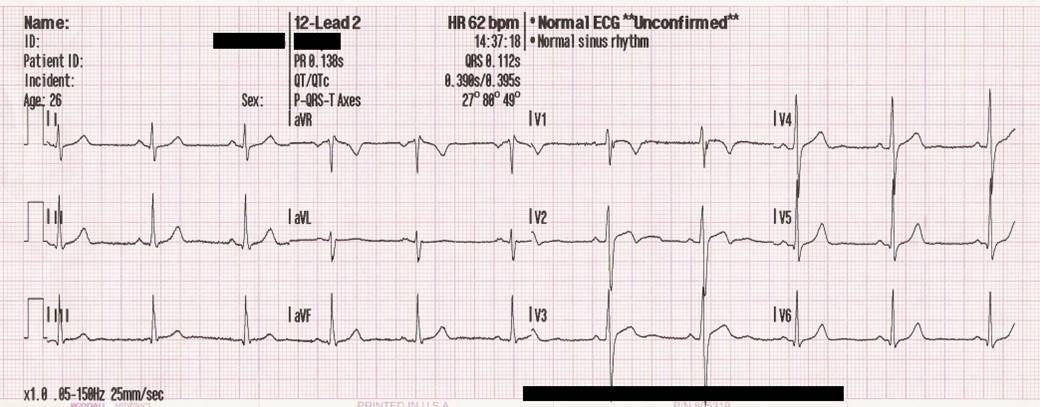
Standard display of ECG leads in the 12-lead ECG
Numerous conditions that can be diagnosed using the 12-lead ECG require that ECG changes occur in two or more anatomically contiguous leads, which implies leads that are anatomically juxtaposed. The reason for this is simple. For example, if there is acute ischemia located in the anterior wall and there is ST segment elevation in lead V3, then there should also be ST elevation in either V2 or V4, because it is unlikely that ischemia would only be detected in one lead. Thus, leads V3 and V4 are anatomically contiguous, as are leads V2 and V3. You have probably noticed that the chest leads (V1 through V6) are displayed on the ECG paper in their anatomically contiguous order from right anterior (V1) to left lateral (V6), but regrettably, the limb leads are not. Instead, the limb leads are displayed in two groups of three: leads I, II and III and leads aVR, aVL and aVF. Figure 1 shows the traditional presentation of the 12-lead ECG. This presentation format is the standard in the United States, the United Kingdom, most parts of Europe, South America, Asia and Africa.
Understanding this discussion requires prior knowledge of the ECG leads. Please refer to the chapter The ECG leads.
The Cabrera format of the 12-lead ECG
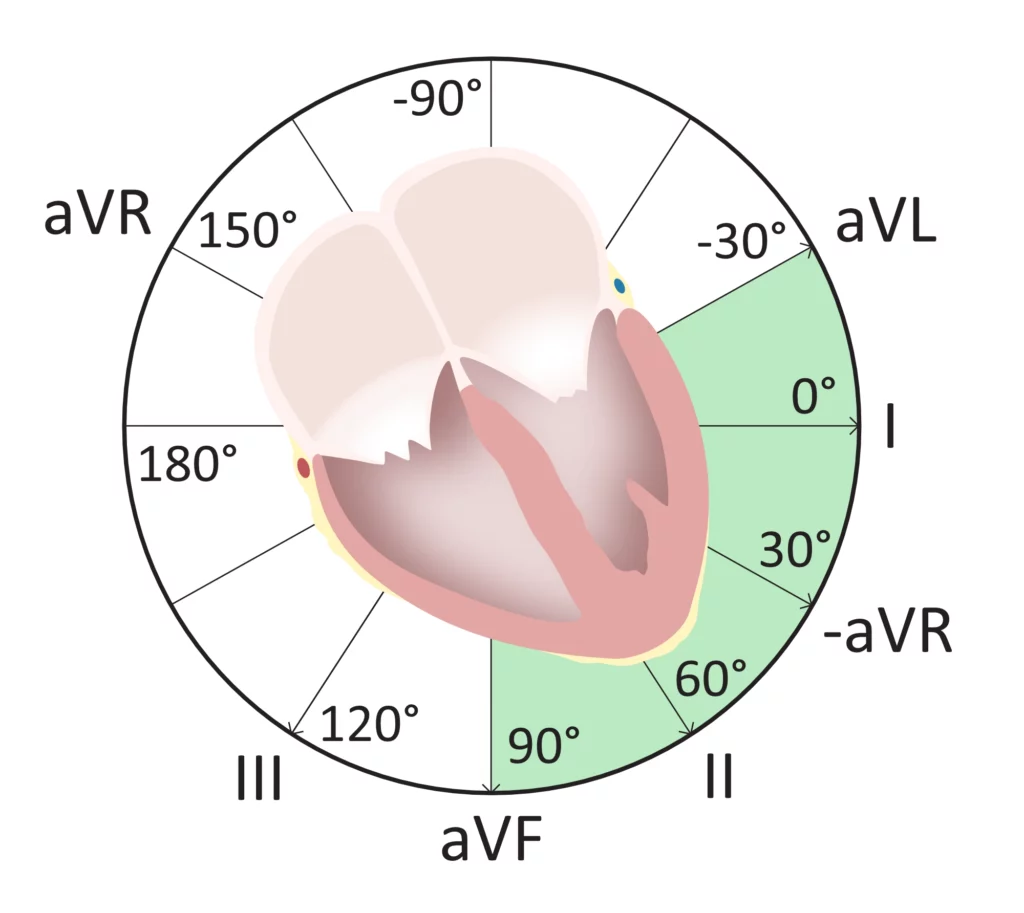
As evident in Figure 1, the traditional presentation of the ECG leads is not particularly helpful. Presentation of leads I, II, III, aVR, aVL and aVF actually reflects their historical development. Leads I, II and III were developed by Einthoven and leads aVR, aVL and aVF were developed by Goldberger. This presentation makes ECG interpretation more difficult and time-consuming, because the reader must go back and forth between the leads on the paper. It would be more efficient to present the limb leads in their anatomically contiguous manner; that is, from left superior-basal to right inferior. In other words, the following order: aVL, I, −aVR (i.e., lead aVR with reversed polarity), II, aVF, and III. Note that lead –aVR exists at 30° in the frontal plane, according to Figure 2.
This format of displaying the ECG leads is referred to as the Cabrera format and it has been the existing standard in Sweden for over 30 years. Let’s have a look at the standard 12-lead ECG with the Cabrera format (Figure 3):
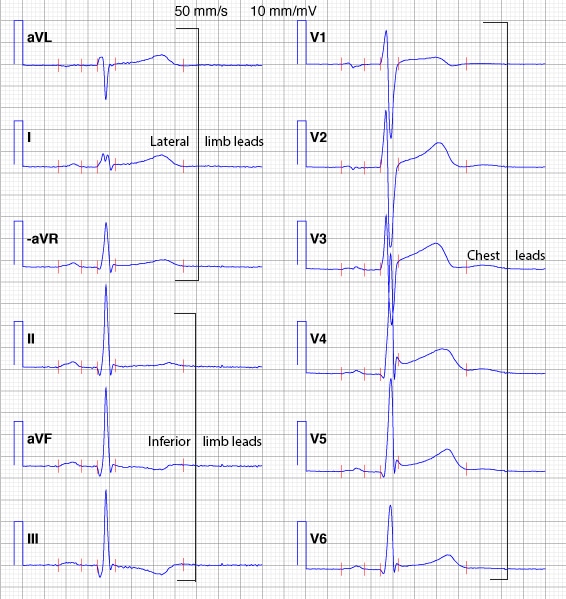
It is easier to study the inferior and lateral walls using the Cabrera format. As evident in Figure 3, if leads I, II and III would have been displayed next to each other, the T-wave inversion in lead III would not be consistent with the upright T-waves in leads I and II. However, placing lead III next to aVF makes more sense, because aVF also displays a negative T-wave.
The American College of Cardiology (ACC), The European Society for Cardiology (ESC), and the American Heart Association (AHA) have recommended that there should be universal adoption of the Cabrera format. This recommendation,1 was issued 16 years ago and fortunately all modern ECG machines can switch to the Cabrera format (including –aVR). We encourage the use of the Cabrera format in order to facilitate ECG interpretation.
Lead –aVR: the inverted lead aVR
As evident in Figure 2 there is a 30° distance between each limb lead, except for the gap between lead I and lead II. To eliminate this gap, lead aVR can be inverted into lead –aVR. To obtain lead –aVR, the exploring and the reference points must switch positions so that lead –aVR is equal to aVR upside-down. It turns out that the use of lead –aVR is meaningful, as it facilitates ECG interpretation (e.g. interpretation of myocardial ischemia and electrical axis). All modern ECG machines can present either aVR or –aVR; we recommend that –aVR be used as it facilitates ECG interpretation. In any case, the reader can easily switch between aVR and –aVR without adjusting the ECG machine; by simply turning the ECG curve upside-down.
Advantages of using lead –aVR instead of aVR
There are three advantages of inverting aVR into –aVR:
- –aVR fills the gap between lead I and lead II in the coordinate system.
- –aVR facilitates the calculation of the heart’s electrical axis.
- –aVR improves diagnosis of acute ischemia/infarction (inferior and lateral ischemia/infarction).
References
Myocardial infarction redefined: a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the Redefinition of Myocardial Infarction. Eur Heart J. 21 2000:1502-1513.
Twelve-lead electrocardiogram: The advantages of an orderly frontal lead display including lead −aVR. Elena B Sgarbossa, MD, S.Serge Barold, MD, Sergio L Pinski, MD, Galen S Wagner, MD, Olle Pahlm, MD, PhD. Journal of Electrocardiology (2006).

