Atrioventricular nodal reentry tachycardia (AVNRT): ECG features & management
Atrioventricular Nodal Reentry (Reentrant) Tachycardia (AVNRT): clinical features, mechanisms, ECG & management
Atrioventricular nodal reentrant tachycardia (AVNRT) is a common tachyarrhythmia observed across all age groups, from children to the elderly, and frequently occurs in otherwise healthy individuals. The arrhythmia is characterized by its abrupt onset and termination and typically presents with symptoms associated with supraventricular tachyarrhythmias, including palpitations, dyspnea, chest discomfort, and anxiety. As the tachyarrhythmia originates above the ventricles, ventricular depolarization proceeds normally via the His-Purkinje system, and in most cases, there is no significant hemodynamic compromise. However, in cases of rapid AVNRT or in patients with underlying structural heart disease, the arrhythmia may result in symptoms indicative of reduced cardiac output, such as pre-syncope or syncope.
Definition of Paroxysmal Supraventricular Tachyarrhythmia (PSVT)
The arrhythmias AVNRT, AVRT (Pre-excitation, Wolff-Parkinson-White syndrome) and ectopic atrial tachycardia have traditionally been referred to as paroxysmal supraventricular tachycardias, because these tachyarrhythmias originate in the atria (hence “supraventricular”) and they tend to be paroxysmal. However, the term PSVT does not have any clinical relevance and it may lead to misunderstanding. Use of the term PSVT is therefore not recommended.
Synonyms for AVNRT
- Atrioventricular nodal reentrant tachycardia
- Atrioventricular nodal reentry tachycardia
- Atrioventricular nodal reentrant tachyarrhythmia
- Atrioventricular nodal reentry tachyarrhythmia
Some textbooks use the term “node” instead of “nodal”. AVNRT should not be confused with AVRT, which is the result of pre-excitation (accessory pathway).
AVNRT is caused by reentry in the atrioventricular (AV) node
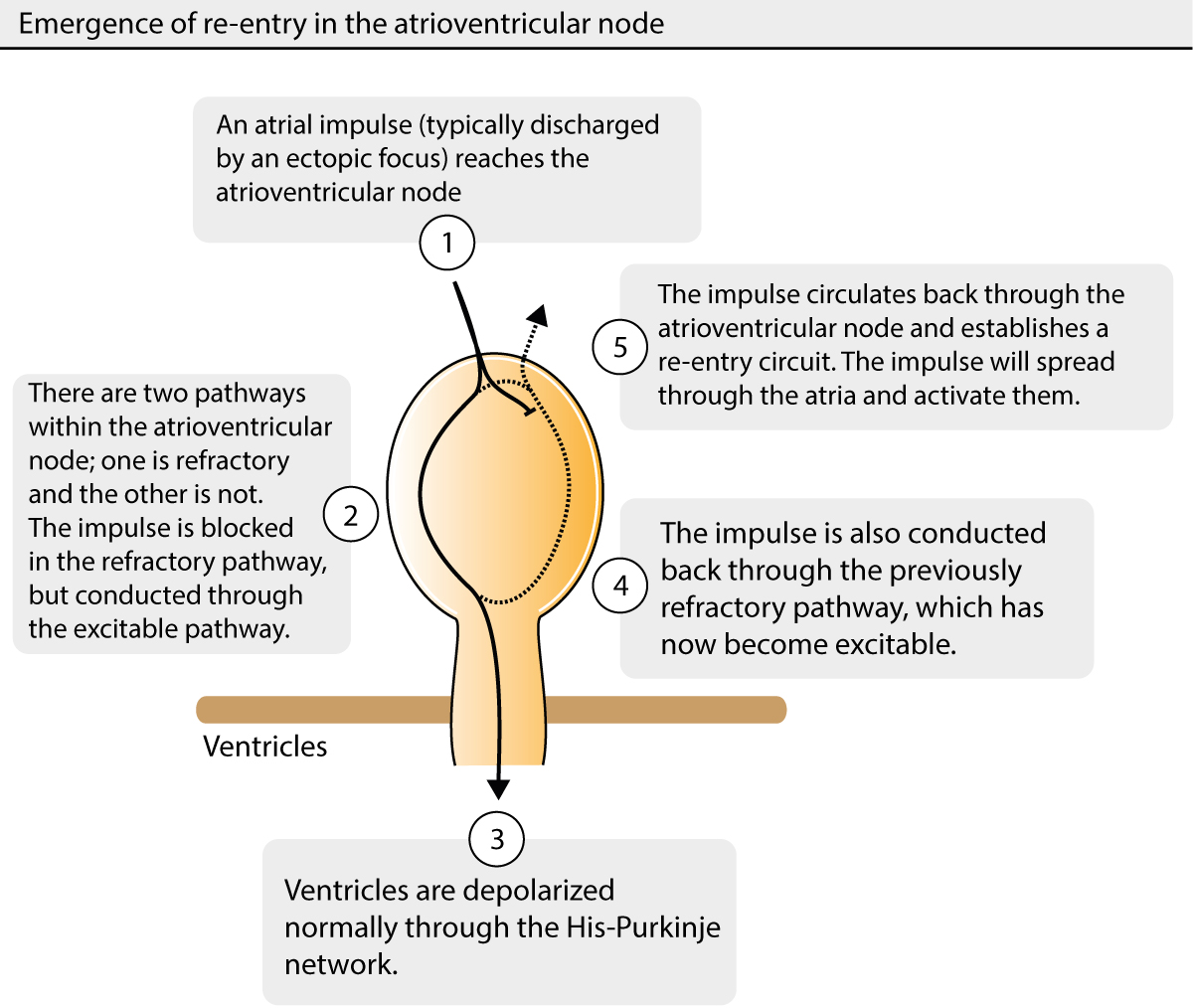
Atrioventricular nodal reentrant tachycardia (AVNRT) is caused by a re-entry within the atrioventricular node. In most cases, the re-entry is induced by a premature atrial beat reaching the atrioventricular node while some fibers are still refractory. If an atrial impulse reaches the atrioventricular node when there are two pathways, one being refractory and the other capable of conducting the impulse, re-entry may arise. This is illustrated in Figure 1 (study this figure carefully). The impulse will only be conducted through the excitable pathway whereas it will be blocked in the refractory pathway. If the refractory pathway has repolarized before the impulse has left the atrioventricular node, it may circulate back (upwards) through the previously refractory pathway, as shown in Figure 1. The impulse may subsequently circulate within the atrioventricular node, as long as it encounters excitable tissue. As it circulates within the node, it emits impulses both upwards to the atria and downwards (via His bundle) to the ventricles. Hence, the ventricles will be activated normally via the His-Purkinje system and therefore the QRS complexes are normal (QRS duration < 0.12 s), unless there is a intraventricular conduction defect. The ventricular rhythm is regular (as is the atrial) with a rate ranging between 150 and 250 beats per minute.
The P-wave is not visible in most cases, because it is hidden within the QRS complex (the atria and the ventricles are activated simultaneously, but ventricular potentials dominate the ECG). In some cases, however, the P-wave will be visible, either before or after the QRS complex. In either case it will be retrograde (in lead II, III and aVF) because of the direction of atrial activation. P-waves in AVNRT are discussed in detail below.
ECG features of Atrioventricular Nodal Reentrant Tachycardia (AVNRT).
There are three types of AVNRT and the difference between them lies in the configuration of the re-entry circuit. Virtually all cases of AVNRT are characterized by having one fast and one slow pathway. Findings on the ECG depend on which of these pathways that lead the impulse in antegrade direction (to the ventricles) and in the retrograde direction (to the atria). The three types of AVNRT are now discussed (illustrated in Figure 2).
Typical AVNRT (slow-fast): 90% of all cases of AVNRT
In typical AVNRT the pathway with antegrade conduction is the slow pathway, whereas retrograde conduction is fast (hence called slow-fast AVNRT). Typical AVNRT occurs when the atrial impulse (typically a premature atrial impulse) reaches the atrioventricular node when the fast pathway is refractory and the slow pathway is excitable (Figure 1 for the mechanism and Figure 2 for ECG example). The impulse is conducted through the slow pathway and before it leaves the atrioventricular node the fast pathway has recovered, such that the impulse may also travel up via the fast pathway. The impulse starts to circulate within the atrioventricular node and a re-entry circuit is established. The re-entry circuit will emit impulses up to the atria and down to the ventricles simultaneously, which is why the P-wave will be hidden within the QRS complex.
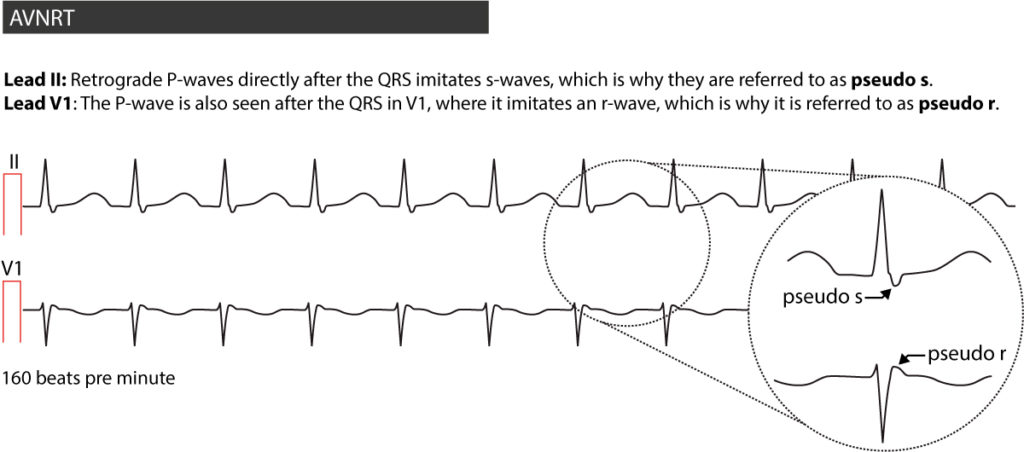
In roughly 25% of slow-fast AVNRT the atria will be activated slightly after the ventricles, which is why the P-wave can be seen right after the QRS complex (often fused with it). The P-wave will be retrograde in lead II, III and aVF; because it is (more or less) fused with the QRS, it will imitate an s-wave and therefore it has been termed pseudo s. The same P-wave is positive in lead V1, where it imitates an r-wave and therefore it has been termed pseudo r. In most cases, a previous ECG recording is needed to verify that these waves do not exist normally. If a previous ECG is not at hand, one could suspect such waves to be P-wave if the waves are smooth (as is the P-wave); ventricular deflections are sharp waves. Refer to Figure 2.
Log in to view image, video, quiz, text

Atypical AVNRT (fast-slow): 10% of all cases of AVNRT
In atypical AVNRT the fast pathway conducts the impulse in antegrade direction while the slow pathway conducts it in the retrograde direction. The P-wave will be visible before the QRS complex. The P-wave will be retrograde in lead II, III and aVF and positive in lead V1. Refer to Figure 2, panel B.
Very atypical AVNRT (slow-slow): <1 % of all cases of AVNRT
In this case, both pathways are slow and the P-wave occurs somewhere on the ST-T-segment. Refer to Figure 2, panel C.
The ECG below shows a recording from a 20-year old male who arrived at the emergency room due to palpitations and dyspnea which started abruptly (Figure 3). The arrhythmia was terminated by administration of 5 mg adenosine i.v.
RP interval (RP time)
The RP interval (i.e the time interval from R-wave to P-wave) is fundamental to assess when managing arrhythmias with visible P-waves. Typical AVNRT has a short RP interval (i.e shorter than half the RP interval). Atypical and very atypical AVNRT has a long RP interval (i.e longer than half the RP interval). Refer to this article to learn about RP interval.
Treatment of AVNRT
Treatment in the emergency setting
Always attempt to terminate the AVNRT by applying vagus stimulation (Valsalva maneuver, carotid massage, or, if the patient is a child, bringing ice-cold water to the face). If vagus stimulation is not successful, adenosine can be administered safely, starting at 5 mg iv. The handling and dosing of adenosine are discussed in a separate article. If adenosine is contraindicated or fails after 2 to 3 repeated administrations, it is reasonable to try verapamil 5–10 mg iv or diltiazem 0.25 mg/kg iv. Almost 90% of all cases of AVNRT will be terminated using this algorithm.
Synchronized electrical cardioversion may be preferred over verapamil and diltiazem. Importantly, electrical cardioversion is the first choice if there are signs of hemodynamic compromise. 10–100 J biphasic shock (synchronized) is usually adequate. Beta-blockers have no place in the acute treatment of AVNRT.
Long-term treatment and prophylaxis
Patients with recurring episodes of AVNRT should be considered for long-term/prophylactic treatment with beta-blockers, calcium channel blockers or digoxin. Radiofrequency ablation cures virtually all patients who are referred for intervention.

