Pulmonary embolism occurs when venous thrombi embolize to the pulmonary artery or its branches. In the majority of cases, the thrombus is formed in the deep veins of the legs or pelvis. Thrombi formed in the deep veins in the legs or pelvis can detach and flow via inferior vena cava to the right atrium and ventricle. The thrombus is pumped from the right ventricle through the pulmonary valve into the main pulmonary artery. Depending on the size and form of the thrombus, it will occlude the main pulmonary artery or its branches. The larger the thrombus, the more proximal the occlusion and, hence, the greater the hemodynamic effects.
The occlusion has two immediate effects:
- Reduced perfusion in the pulmonary circulation, resulting in hypoxia.
- Reduced preload in the left ventricle and consequently reduced cardiac output.
A substantial reduction in pulmonary perfusion and the subsequent reduction in left ventricular preload lead to a cascade of hemodynamic alterations which may culminate in cardiac arrest.
Pulmonary embolism is causally related to deep vein thrombosis (DVT). Approximately 70% of individuals with symptomatic pulmonary embolism have an ongoing DVT, and 30% of individuals with DVT have asymptomatic pulmonary emboli (Di Nisio et al). Accordingly, risk factors for pulmonary embolism overlap with risk factors for DVT; immobilisation, surgery, hypercoagulability, and pregnancy are common risk factors (see Risk factors below).
A significant proportion of cases with pulmonary embolism require thrombolysis to dissolve the occlusion. Administration of thrombolysis requires careful consideration of absolute and relative contraindications (discussed below), and assessment of differential diagnoses; cardiac tamponade, aortic aneurysm and aortic dissection are common differential diagnoses which represent contraindications for thrombolysis.
Venous thromboembolism is a chronic and serious condition. Mortality in pulmonary embolism is up to 20%, and roughly 30% of patients with pulmonary embolism or deep vein thrombosis experience a second thrombotic event within 10 years (Goldhaber et al, Kearon et al).
Epidemiology of pulmonary embolism
- Venous thromboembolism (VTE) is the third leading cardiovascular cause of death worldwide. Only stroke and acute myocardial infarction are more common. It is estimated that 10 million cases of venous thromboembolism occur globally every year (Raskob et al).
- The incidence of pulmonary embolism has increased in recent decades. Potential explanations for this trend include an ageing population, increased incidence and prevalence of cancer, heart failure, obesity, type 2 diabetes and physical inactivity. The increased use of computed tomography (CT), and improvements in CT techniques, have increased the detection of pulmonary embolism.
- Currently, the lifetime risk of developing venous thromboembolism is 8% for individuals 45 years of age (Raskob et al, Heit et al).
Cardiopulmonary effects of pulmonary embolism
Hemodynamic effects
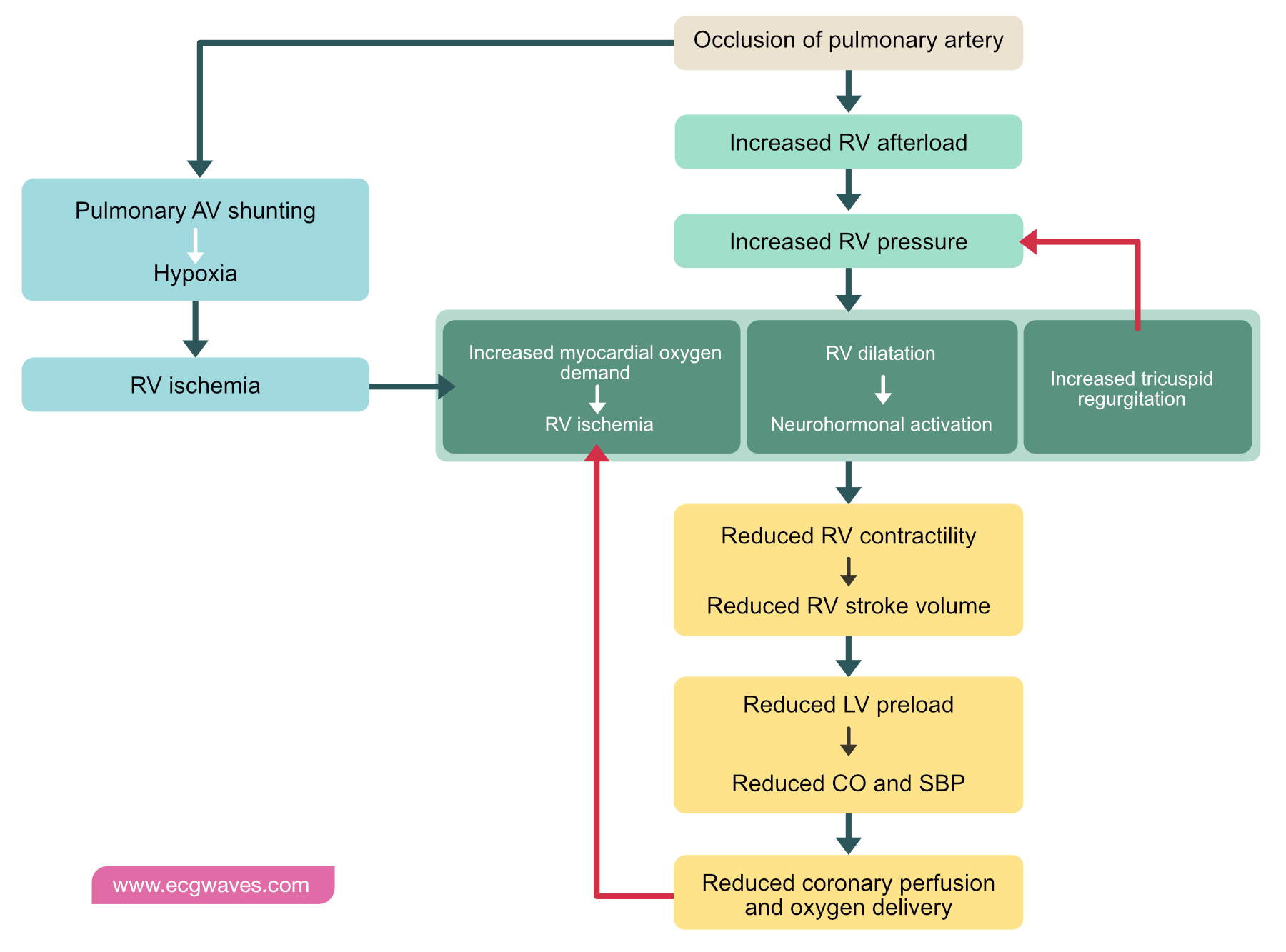
Pulmonary embolism leads to increased resistance in the main pulmonary artery, and thereby increased afterload on the right ventricle. This increases the load on the right ventricle, which therefore requires more oxygen. The increase in afterload also results in increased intramural pressure in the right ventricle, which is counteracted by dilatation of the ventricle. Dilatation of the right ventricle results in reduced intraventricular pressure and thereby reduced myoardial load.
Pulmonary embolism causes increased right ventricular load, which results in increased oxygen demand and dilatation of the right ventricle.
Despite the dilation, myocardial ischemia will develop if right ventricular oxygen demand exceeds oxygen delivery. Prolonged and pronounced ischemia leads to right ventricular infarction. Whether infarction develops or not, the dilatation, increased afterload and ischemia results in reduced right ventricular stroke volume. As right ventricular stroke volume diminishes, less blood is pumped into the left ventricle, leading to decreased left ventricular preload. Declining preload leads to a decrease in cardiac output and a subsequent drop in systolic blood pressure. Reduced cardiac output and reduced blood pressure yields a reduction in coronary perfusion pressure, including perfusion through the right coronary artery (RCA). This further aggravates ischemia in the right ventricle. Right ventricular stroke volumes decline more, leading to further reductions in left ventricular preload and the cycle repeats itself.
The gradual drop in cardiac output, systolic blood pressure and coronary perfusion will ultimately result in cardiac arrest, typically with pulseless electrical activity (PEA) on ECG.
Acute right ventricular load is also referred to as right ventricular strain.
Pulmonary effects
Obstruction of pulmonary arteries leads to hypoxia in lung parenchyma and pleura. Prolonged hypoxia results in parenchymal inflammation and ultimately infarction (i.e pulmonary infarction). This manifests with chest pain; typically pleuritic chest pain (sharp pain correlated to respiration). Lung infarction leads to parenchymal hemorrhage, which manifests with hemoptysis.
The occlusion also leads to ventilation-perfusion mismatch (i.e there are ventilated areas that are not perfused), resulting in reduced oxygenation of blood. This results in decreased arterial oxygen pressure (PaO2) and oxygen saturation (hypoxia). Reflex hyperventilation may lead to respiratory alkalosis with hypocapnia (reduced PaCO2).
Symptoms and signs of pulmonary embolism
The majority of cases with pulmonary embolism have acute onset of symptoms. Onset may be related to changes in body position or physical activity. It can be presumed that the activity or change in body position causes dislodgement of venous thrombi, which then travel to the heart.
Symptoms depend on hemodynamic effects of the occlusion, which is determined by the size and location of the embolus, cardiac function and comorbidites. Small pulmonary emboli may be asymptomatic, while large proximal occlusions may rapidly cause circulatory collapse and cardiac arrest.
The most common symptoms and signs in pulmonary embolism are as follows:
- 50% have dyspnea and tachypnea.
- 50% have chest pain, typically pleuritic chest pain.
- Tachycardia is the most common ECG finding (se ECG in pulmonary embolism below).
- Distended jugular vein (due to elevated right ventricular pressure).
- Cough.
- Hemoptysis.
- Hypotension.
- Substantial drop in systolic blood pressure.
- Syncope, pre-syncope.
- Fever.
- Signs of deep vein thrombosis (DVT) or other venous thrombosis.
Hypotension, drop in systolic blood pressure, pre-syncope or syncope are strong predictors of massive pulmonary embolism.
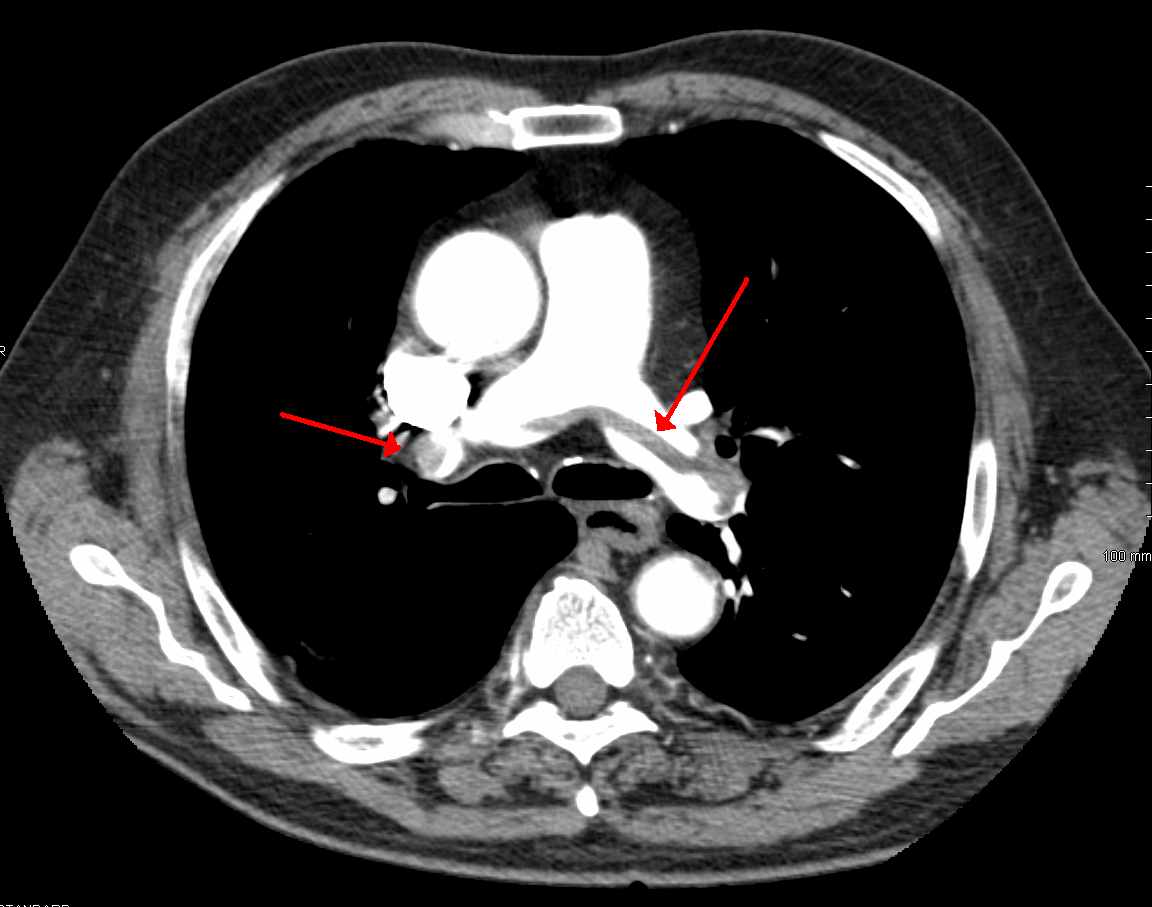
Saddle pulmonary embolism
Saddle pulmonary embolism refers to a large embolus that straddles the bifurcation of the pulmonary trunk, with parts of the embolus extending into the left and right pulmonary arteries. The contour of the embolus on CT scans may resemble a horse saddle (Figure 1). Saddle emboli cause severe hemodynamic effects.
Causes of pulmonary embolism
The most common causes of pulmonary embolism are as follows:
- Deep vein thrombosis (DVT) is the most common cause.
- Fat embolism occurs after surgery, including orthopedic interventions.
- Cement embolism refers to embolization of polymethyl methacrylate (PMMA) into the pulmonary arteries. PMMA is primarily used in percutaneous vertebroplasty.
- Air embolism.
- Amniotic fluid embolism.
- Tissue embolism.
- Tumor embolism.
- Bacterial embolism.
Risk factors for pulmonary embolism
Risk factors of pulmonary embolism are as follows (Di Nisio et al):
Hypercoagulability
- Increasing age
- Cancer
- Antiphospholipid syndrome
- Estrogen therapy
- Pregnancy
- Post-partum period (8 weeks)
- Heredity for venous thromboembolism
- Obesity
- Dehydration
- Inflammatory Bowel Disease (Crohn’s Disease, Ulcerative Colitis)
Interventions and trauma
- Surgery
- Trauma
- Fractures
- Implantation of devices (e.g central venous catheter, pacemaker, ICD, CRT).
Immobilization and hospitalization
- Hospitalization
- Long travel (>3 hours sitting)
- Paralysis, paresis
Hereditary disorders
- Factor V Leiden mutation
- Prothrombin mutation
- Antithrombin mutation
- Protein C deficiency
- Protein S deficiency
Genetic hypercoagulability should be suspected if the patient is young, lacks risk factors for thromboembolism, has heredity or experiences recurring emboli.
Note that 30-50% of all venous thromboembolism is unprovoked. The remained are provoked by one or multiple factors listed above.
Disgnosis of pulmonary embolism

Pre-test probability for pulmonary embolism
Pre-test probability is a statistical term used to guide treatments and investigations. If the pre-test probability of pulmonary embolism is very high, then it is very likely that the patient has pulmonary embolism, making it unnecessary to analyse D-dimer. Similarly, if pulmonary embolism is not likely, then CT scan may not be justified unless D-dimer is positive (elevated). Pre-test probability is assessed in all patients with suspected pulmonary embolism.
Pre-test probability of pulmonary embolism is assessed with one of the following prediction models (scores):
- Wells score
- Modified Wells score
- Revised Geneva score
- PERC (pulmonary embolism rule-out criteria)
Wells score and modified Wells score can be used in inpatient and outpatient settings. PERC is used to exclude pulmonary embolism.
If clinical suspicion of pulmonary embolism is high, the patient should undergo computed tomographic scan, regardless of scores and D-dimer.
Wells score for pulmonary embolism
Wells score for pulmonary embolism should not to be confused with Wells score for DVT. The below risk model (score) is only used in case of suspicion of pulmonary embolism.
Table 1. Wells criteria for pulmonary embolism
| CRITERIA | POINTS |
|---|---|
| Symptoms or signs of DVT | 3 |
| Pulmonary embolism more likely than other diagnoses | 3 |
| Previous VTE (PE or DVT) | 1.5 |
| Tachycardia (HR >100/bpm) | 1.5 |
| Immobilization or surgery in the past 4 weeks | 1.5 |
| Hemoptysis | 1 |
| Cancer | 1 |
Evaluation of Wells score
Wells score, original
- 0-1 points: Low probability (6% absolute risk).
- 2 to 6 points: Intermediate probability (23% absolute risk)
- ≥7 points: High probability (50% absolute risk)
Wells score, modified
- ≤ 4 points: Pulmonary embolism not likely (8% absolute risk)
- ≥ 5 points: Pulmonary embolism likely (34% absolute risk).
Revised Geneva score for pulmonary embolism
Table 2. Revised Geneva score for pulmonary embolism
| CRITERIA | POINTS |
|---|---|
| Age >65 years | 1 |
| Previous VTE (PE or DVT) | 3 |
| Recent surgery (any) or lower extremity fracture | 2 |
| Cancer | 2 |
| Unilateral leg pain | 3 |
| Hemoptysis | 2 |
| Heart rate 75–94 bpm | 3 |
| Heart rate ≥ 95/min | 5 |
| Pain on palpation of lower limb with unilateral edema | 4 |
Evaluation of Geneva score
- <4 points: low probability of pulmonary embolism (9% absolute risk)
- 4 to 10 points: intermediate probability of pulmonary embolism (26% absolute risk)
- >10 points: high probability of pulmonary embolism (76% absolute risk)
Pulmonary Embolism Rule-Out Criteria (PERC)
If the probability of pulmonary embolism is low (according to Wells score or Geneva score), then PERC can be used to exclude pulmonary embolism.
Table 3. Pulmonary Embolism Rule-Out Criteria (PERC)
| CRITERIA | POINTS |
|---|---|
| Age > 50 years | 1 |
| Heart rate > 100/min | 1 |
| Oxygen saturation (POX) < 95% | 1 |
| Hemoptysis | 1 |
| Estrogen therapy | 1 |
| Previous VTE (PE or DVT) | 1 |
| Recent (<4 weeks) surgery (any) or trauma | 1 |
| Unilateral lower limb edema | 1 |
Evaluation of PERC score
- 0 points: low probability (< 1%). Pulmonary embolism very unlikely.
- ≥1 point: pulmonary embolism is not excluded and further investigation is required.
D-dimer
D-dimer is a byproduct produced during degradation of fibrinogen. Hence, elevated D-dimer levels indicate recent fibrinolysis.
D-dimer is analyzed if the probability of pulmonary embolism is low to intermediate. D-dimer has very high sensitivity for venous thromboembolism, including pulmonary embolism; virtually all patients with pulmonary embolism exhibit with elevated D-dimer levels. However, specificity is low, which is due to the fact that D-dimer levels increase in all situations with thrombosis.
Negative D-dimer excludes pulmonary embolism (and DVT) if clinical suspicion is low to intermediate. If clinical suspicion of pulmonary embolism is high, then D-dimer must not be used to exclude pulmonary embolism.
Other biomarkers
- Electrolytes, renal function (estimated GFR) and liver function must be assessed in all patients.
- Troponin (troponin T, troponin I) is analyzed to determine whether myocardial infarction has occurred. Increased troponin levels indicate right ventricular infarction, which is prognostically unfavourable.
- Blood (arterial) gas is not necessary to analyze. Results typically show resporatory alkalosis, reduced oxygen pressure (PaO2) and elevated pH.
ECG in pulmonary embolism
The ECG can be used to find additional signs of pulmonary embolism. Sensitivity and specificity are low for all ECG criteria proposed for detection of pulmonary embolism.

The following ECG changes may be seen in pulmonary embolism:
- S1Q3T3 pattern refers to the presence of a deep S-wave in lead I and a deep Q-wave in lead III, and T-wave inversion in lead III.
- T-wave inversions (negative T-waves) in V1-V4.
- New onset complete or incomplete right bundle branch block (RBBB).
- New onset atrial fibrillation, atrial flutter or atrial tachycardia.
- ST elevation or ST depression in V1-V3.
- P pulmonale
- Right axis deviation (RAD).
Sinus tachycardia is the most common ECG finding in pulmonary embolism.
Computed tomography of the pulmonary arteries (CTPA)
Computed tomography of the pulmonary arteries (CTPA) is the preferred imaging method in suspicion of pulmonary embolism. The study, which is contrast-enhanced, is fast, has high sensitivity and high specificity.
Acute pulmonary embolism is diagnosed when CTPA shows complete or partial filling defects in the pulmonary arteries. Partial filling defects can be centrally or peripherally located within the artery and will be surrounded by contrast (Leitman et al).
Indirect signs of pulmonary embolism include pleural fluid or wedge-shaped pulmonary infarction.
Computed tomography should be avoided in the following situations:
- Pregnancy.
- Contrast allergy.
- Renal failure.
Lung scintigraphy
Lung scintigraphy is performed if CTPA is inappropriate due to pregnancy, contrast allergy or renal failure. Scintigraphy is time-consuming and requires low doses of radioactive markers. Pulmonary perfusion is compared with pulmonary ventilation and any regional discordance, referred to as mismatch, in ventilation and perfusion is suggestive of pulmonary embolism.
Echocardiography
Echocardiography is recommended to visualize indirect signs of pulmonary embolism and right ventricular strain. The following echocardiographic findings suggest acute pulmonary embolism:
- Increased tricuspid regurgitation (TI).
- Increased PASP (systolic PA pressure).
- Dilated vena cava inferior, with loss of respiratory variation.
- Right ventricular dilatation.
- Paradoxical septal movement.
Other imaging methods
Pulmonary angiography is performed in selected cases, especially if endovascular therapy is feasible.
Magnetic resonance imaging has high sensitivity and specificity and can be performed if the diagnosis is unclear or if other modalities are not feasible.
Treatment of pulmonary embolism

In the acute setting, treatment is guided by the patient’s hemodynamic condition. Severe pulmonary embolism (massive pulmonary embolism) is managed with immediate anticoagulation and reperfusion (thrombolysis). Pulmonary embolism without hemodynamic effects is treated with anticoagulants.
Severe (massive pulmonary embolism) is defined as pulmonary embolism that meets any of the following criteria:
- Systolic blood pressure <90 mm Hg
- >40 mm Hg drop in systolic blood pressure.
There are, however, additional warning signs:
- Syncope, pre-syncope, dizzyness.
- Tachycardia.
- Right ventricular dilation, elevated PASP.
- Paradoxical septal movement.
- Elevated BNP or NT-proBNP or troponin.
Risk stratification of pulmonary embolism: PESI (Pulmonary Embolism Severity Index)
PESI estimates 30-days mortality among patients with confirmed pulmonary embolism. PESI is used to guide initial management.
Table 4. PESI (Pulmonary Embolism Severity Index)
| CRITERIA | POINTS |
|---|---|
| Age | 1 per year |
| Cancer | 30 |
| Systolic blood pressure < 100 mm Hg | 30 |
| Heart rate ≥ 110/min | 20 |
| Oxygen saturation (POX) < 90% | 20 |
| Heart failure | 10 |
| Pulmonary disease | 10 |
| Altered mental status | 60 |
| Body temperature <96.8°F or < 37°C | 20 |
| Respiratory rate ≥ 30/min | 20 |
| Male sex | 10 |
Evaluation of PESI score
| PESI CLASS | PESI POINTS | RISK | 30-DAYS MORTALITY | IN-HOSPITAL MORTALITY |
|---|---|---|---|---|
| Class I | <66 | Very low risk | 0–1.6% | ≤1.1% |
| Class II | 66-85 | Low risk | 1.7–3.5% | ≤1.9% |
| Class III | 86–105 | Intermediary risk | 3.2–7.1% | ≤4.7% |
| Class IV | 106–125 | High risk | 4.0–11.4% | ≤7.0% |
| Class V | > 125 | Very high risk | 10.0–23.9% | ≤17.2% |
Treatment of high risk (massive) pulmonary embolism
High risk pulmonary embolism (30-days mortality >15%) is synonymous with massive pulmonary embolism. These patients have systolic blood pressure <90 mm Hg, alternatively >40 mm Hg drop in systolic blood pressure. The vast majority of these patients need thrombolysis. Rapid echocardiography (TTE) and CT scan are important.
Immediate actions
- Start infusion with low molecular weight heparin (e.g enoxaparin).
- Administer oxygen if oxygen saturation <95%.
- Consider administering fluid bolus (500 ml).
- Provide inotropic support (e.g norepinephrine) if hypotensive.
- Determine whether there are contraindications to thrombolysis. If no contraindications are present, alteplas is given:
- Alteplas i.v 10 mg in 2 min and 90 mg infusion in 120 minutes.
- Max dose is 1.5 mg/kg for patients weighing <65 kg.
- Heparin infusion is paused during thrombolysis and reinstated at earliest 60 minutes after completion of alteplas infusion.
Catheter based local thrombolysis or thrombectomy may be preferred in specific situations, or if thrombolysis fails to yield reperfusion. Surgical thrombectomy may also be considered, depending on local routines.
Contraindications to thrombolysis
Absolute contraindications
- Structural intracranial disease
- Previous cerebral hemorrhage
- Previous ischemic stroke <3 months
- Ongoing bleeding
- Recent spinal or cardiac surgery
- Head trauma or brain injury
- Hypocoagulability
Relative contraindications to thrombolysis
- Systolic blood pressure >180 mm Hg or diastolic >110 mm Hg
- Recent bleeding (not intracranial)
- Recent surgery (other than cardiac, spinal)
- Recent invasive procedure
- Ischemic stroke >3 months ago
- Use of anticoagulants
- Pericardial effusion
- Diabetic retinopathy
- Pregnancy
- Age >75 Years
- Body Weight <60 kg
Treatment of low to intermediate risk pulmonary embolism
Low to intermediate risk pulmonary embolism is managed with novel oral anticoagulants (NOAC). NOACs result in 30% lower risk of serious bleeding events, as compared with warfarin. The following principles apply to management of patients with pulmonary embolism:
Initial treatment
- If dabigatran or edoxaban are selected for long-term treatment, 5 days initial treatment with low molecular weight heparin (LMWH) is required.
- If rivaroxaban or apixaban are selected for long-term treatment, pre-treatment with LMWH is not needed.
- Suitable LMWH includes enoxaparin for patients with normal renal function. Patients with renal failure are treated with unfractionated heparin (UFH). UFH is also preferred in patients who may later require thrombolysis.
- LMWH is preferred as the initial and long-term treatment in pregnant women and individuals with cancer.
Long-term treatment
- LMWH is preferred in pregnant women and individuals with cancer.
- For warfarin, therapeutic PK-INR is 2 to 3.
- NOAC doses:
- Dabigatran: 150 mg x 2
- Edoxaban: 60 mg x 1
- Rivaroxaban: 15 mg x 2 for 21 days, then 20 mg x 2
- Apixaban: 10 mg x 2 for 7 days, then 5 mg x 2.
Evaluation of bleeding risk
No specific risk model has been developed for pulmonary embolism. HAS-BLED is frequently used, despite the fact that it was validated to assess bleeding risk in patients with atrial fibrillation. Risk factors for bleeding include the following:
- High age
- Frailty
- Previous bleeding events
- Cancer
- Renal failure
- Liver failure
- Thrombocytopenia
- Stroke
- Diabetes
- Anemia
- Treatment with platelet inhibitors or anticoagulants.
- Recent surgery
Long-term complications of pulmonary embolism
- Pulmonary hypertension develops in <5%.
- Cardiac arrest.
- Right ventricular failure (see Heart failure).
- Pulmonary infarction (10% of cases).
- Pleural effusion
- Post-thrombotic syndrome (30%).
References
Di Nisio et al. Deep vein thrombosis and pulmonary embolism. Lancet 2016;388:3060-73
Raskob GE, Angchaisuksiri P, Blanco AN, et al. Thrombosis:
a major contributor to global disease burden. Arterioscler Thromb Vasc Biol 2014; 34: 2363–71
Heit JA. Epidemiology of venous thromboembolism. Nat Rev Cardiol 2015; 12: 464–74.
Kearon C et al. Natural history of venous thromboembolism. Circulation 2003; 107: I22–30.
Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet 1999; 353: 1386–89.
Konstantinides et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society. European Heart Journal (2020) 41, 543603.
Leitman et al. Pulmonary arteries: imaging of pulmonary embolism and beyond. Cardiovasc Diagn Ther. 2019 Aug; 9(Suppl 1): S37–S58

