ECG changes due to electrolyte imbalance (electrolyte disorder)
The normal cardiac action potential may be altered by electrolyte imbalance, owing to changes in intra- and extracellular electrolyte concentrations. Some electrolyte imbalances are clinically negligible (from an electrophysiological standpoint), whereas others may be life-threatening. The most common and clinically most relevant electrolyte imbalances concern potassium, calcium and magnesium. Note that some patients may exhibit combined electrolyte imbalance. The ECG may be used to estimate the severity of electrolyte imbalances and to judge whether there is a risk of serious arrhythmias. This is possible because there is a correlation between the severity of electrolyte imbalance and the visible ECG changes.
Specific electrolyte disorders
1. Sodium
Increased (hypernatremia) and decreased (hyponatremia) sodium levels do not have any effect on the ECG, nor cardiac rhythm, or impulse conduction.
2. Calcium
Hypercalcemia
Causes of hypercalcaemia
Primary hyperparathyroidism and malignancies cause 90% of all cases of hypercalcemia. Less common causes are immobilization, sarcoidosis, thyrotoxicosis, familial hypocalciuric hypercalcemia, Addison’s disease, renal failure, tamoxifen, lithium, thiazide diuretics, D vitamin and calcium overdose.
ECG changes due to hypercalcemia
- Common ECG changes
- Shortened QT interval.
- Lengthened QRS duration.
- Bradycardia may occur.
- Rare ECG changes
- Increased QRS amplitude.
- Diminished T-wave amplitude
- Osborn-like waves.
- ST segment elevation in leads V1–V2.
- All degrees of AV block.
- Sinus node dysfunction and tach-brady syndrome.
- Ventricular tachycardia, ventricular fibrillation and torsade de pointes.
Hypocalcemia
Causes of hypocalcemia
Acute pancreatitis, pancreas surgery, alkalosis (hyperventilation), rhabdomyolysis, septicemia (sepsis), osteolytic cancer metastases, abnormal calcium absorption (gastrointestinal) and resorption (from primary urine), renal failure, small bowel syndrome, parathyroid gland surgery, use of bisphosphonates, excess calcitonin, use of phenytoin, use of phosphate substitution, use of foscarnet.
ECG changes due to hypocalcemia
- Common ECG changes
- Lengthened QT interval (torsade de pointes is uncommon)
- Shortened QRS duration (has no clinical significance)
- Rare ECG changes
- AV block.
- Sinus bradycardia.
- Sinoatrial (SA) block.
- Ventricular fibrillation.
3. Potassium
Potassium plays a key role in both depolarization and repolarization, which is why potassium imbalance may cause dramatic ECG changes. These are of utmost clinical significance. There is a rather strong correlation between plasma potassium level and ECG changes, as well as the risk of arrhythmia. Therefore the ECG may be used to estimate the severity of hyperkalemia.
Hyperkalemia
Hyperkalemia decreases impulse transmission in the entire heart. Severe symptoms occur at 7 mmol/L or higher.
Causes of hyperkalaemia
Severe hyperkalemia is usually the result of several interacting factors, such as renal failure, insufficient corticosteroid substitution, acidosis, hemolysis and massive muscle damage. Potassium substitution may be the etiology. Potassium-sparing diuretics, ACE inhibitors and angiotensin receptor blockers (ARBs) may also cause hyperkalemia. Insulin deficiency, Addison’s disease and digoxin intoxication may also cause hyperkalemia.
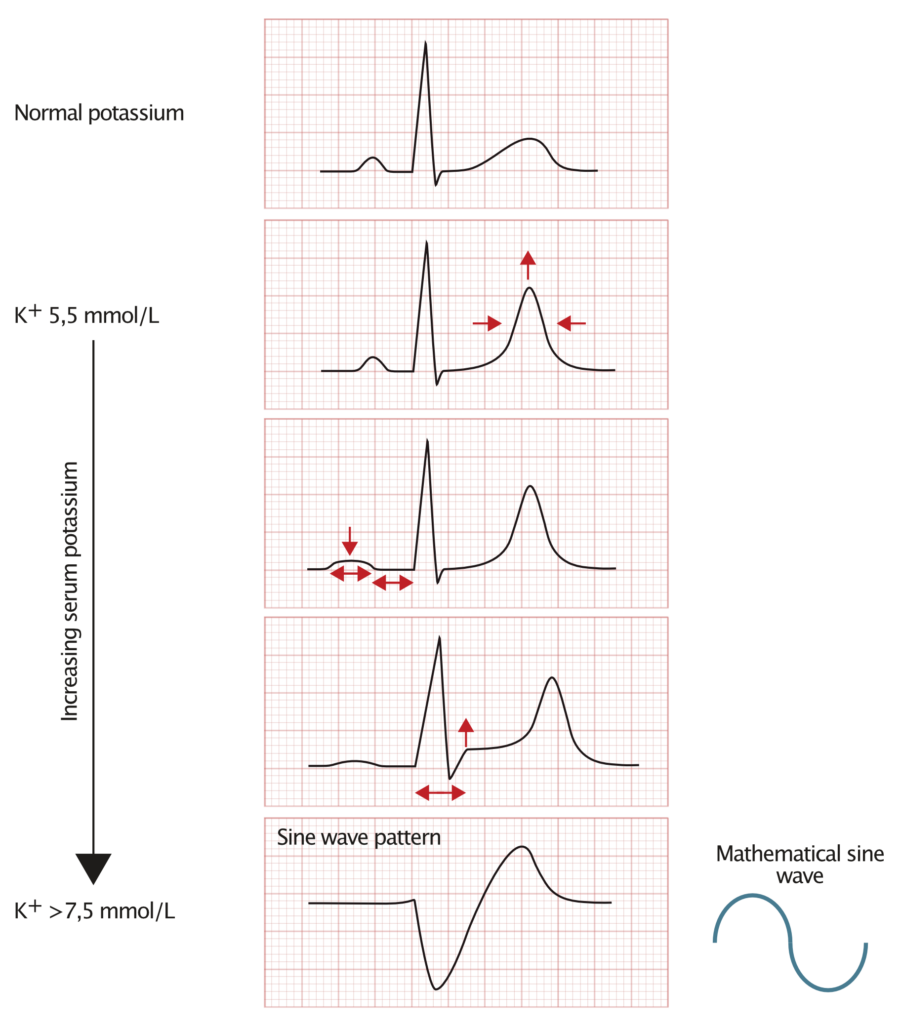
ECG in mild hyperkalemia (potassium >6,0 mmol/L)
- The earliest sign of hyperkalemia is the pointed T-waves. This is most pronounced in the precordial (chest) leads. Pointed T-waves are tall and narrow at the top. Refer to Figure 1.
- Patients with left ventricular hypertrophy may instead display normalization of secondary T-wave inversions (lead V5, V6, aVL, I).
ECG in moderate hyperkalaemia
- Previously mentioned ECG changes becomes more pronounced.
- P-waves become wider. P-wave amplitude decreases. The P-wave may be difficult to discern. Refer to Figure 1.
- The PR interval is prolonged. Occasionally sinoatrial (SA) block, second- or third-degree atrioventricular (AV) block may develop.
- Patients with WPW syndrome may lose their delta wave because of ceased transmission through the accessory pathway.
- ST segment elevation may occur in V1–V3.
ECG in severe hyperkalemia (Potassium >7,5 mmol/L)
- Previously mentioned ECG changes become more pronounced.
- The QRS complex becomes wider. Refer to Figure 1.
If the hyperkalemia is very severe, the QRS complex may fuse with the T-wave and form a so-called sine wave. This is certainly alarming because sine wave pattern usually precedes ventricular fibrillation.
Hypokalemia
Serious complications may occur at 3 mmol/L and below.
Causes of hypokalemia
Diarrhea, excess vomiting, alcoholism, malnutrition, acute medical illness, primary or secondary aldosteronism, excess intake of licorice, glucose infusion, diuretics, adrenergic agonists, theophyllamine, corticosteroids, insulin.
ECG changes in hypokalemia
The following ECG changes occur in chronological order as potassium levels decrease.
- T-waves become wider with lower amplitudes. T-wave inversion may occur in severe hypokalemia.
- ST segment depression develops and may, along with T-wave inversions, simulate ischemia.
- P-wave amplitude, P-wave duration and PR interval may all increase.
- Finally, U-waves emerge. U-waves are best seen in leads V2–V3. If the hypokalemia is severe, the U-wave may become larger than the T-wave.
Hypokalemia may cause acquired long QT syndrome (LQTS) and predisposes to torsade de pointes (polymorphic ventricular tachycardia). Hypokalemia may also cause monomorphic ventricular tachycardia.
Hypokalemia potentiates the pro-arrhythmic effects of digoxin.
4. Magnesium
Hypermagnesemia is rare but severe hypermagnesemia may cause atrioventricular and intraventricular conduction disturbances, which may culminate in third-degree (Complete) AV block or asystole.
Hypomagnesemia may potentiate the pro-arrhythmic effect of digoxin. Hypomagnesemia may also predispose to supraventricular and ventricular tachyarrhythmias.

