Interpretation of neonatal and pediatric electrocardiograms (ECG)
Definition of normal and pathological pediatric and neonatal ECG
The neonatal and pediatric electrocardiogram (ECG) is interpreted using the same principles as in ECG interpretation in adults. The ECG must always be interpreted using a systematic approach in order to minimize the probability of missing significant abnormalities. The following parameters must be assessed, in chronological order:
- Heart rate
- Rhythm
- P-wave
- PR interval
- QRS complex
- ST-segment
- T-wave
- U-wave
- QT (QTc) interval
Pediatric and neonatal electrocardiograms differ markedly – in terms of rhythm, morphology, normal findings, normal variants, etc – from adult electrocardiograms. It is crucial to be familiar with normal findings, normal variants, and pathology in neonates, infants and during the childhood years. Below follows a discussion on each of the nine parameters listed above. Many of the diagnoses mentioned below are discussed in detail in other chapters, to which links are provided throughout the text.
Heart rate
During the first week of life, the heart rate is approximately 120 beats/min. The heart rate then increases during the first 1 to 2 months to about 150 beats/min. It then gradually decreases to about 120 beats/min at 6 months of age. After 12 months of age, the heart rate is steadily decreasing, and by age 10 years the rate is the same as in adults. These age variations in heart rate are due to variations in the activity of the autonomic nervous system and changes in the automaticity of the sinoatrial node.
Rhythm
Normal rhythm
A rhythm is defined as three consecutive beats with identical waveforms on the ECG. The similarity of the waveforms indicates that the origin of the impulse is the same. The sinoatrial (SA) node is the heart’s pacemaker under normal circumstances and the rhythm is referred to as sinus rhythm. Hence, sinus rhythm is the normal rhythm of the heart. Sinus rhythm is the normal rhythm in all pediatric patients. Sinus rhythm is defined by the following criteria:
- Regular rhythm with a ventricular rate within the age-specific normal interval.
- P-wave with constant morphology preceding every QRS complex.
- The P-wave is positive in lead II (and also I and aVF).
Arrhythmias
Sinus tachycardia
Sinus tachycardia exists if the heart rate is higher than the upper normal limit. Sinus tachycardia can exceed 240 beats/min in children. As in sinus rhythm, a P-wave precedes every QRS complex and the P-wave is positive in lead II.
Sinus tachycardia is always considered pathological and the underlying cause must be investigated. Pain, infections, medications, fever, hypovolemia, dehydration, anemia, hyperthyroidism and myocarditis are common etiologies. Treatment of the underlying cause should resolve the sinus tachycardia.
Sinus arrhythmia
Sinus arrhythmia (respiratory sinus arrhythmia) fulfills all criteria for sinus rhythm except for the fact that the rhythm is slightly irregular. The phenomenon is explained by variations in heart rate caused by respiration. The heart rate increases during inspiration (due to diminished vagal tone) and decreases during expiration (due to increased vagal tone). This results in a slightly irregular rhythm.
Sinus arrhythmia occurs in the majority of healthy pediatric patients. P-waves precede all QRS complexes and the PR interval is constant. Although sinus arrhythmia can be pronounced in pediatric patients, it is considered a benign finding.
Generally, sinus arrhythmia is more pronounced in older children because they have a lower heart rate. Older children may be asked to hold their breath, which leads to the cessation of sinus arrhythmia.
Sinus pause
Sinus pause also occurs in children. It manifests in the form of sudden prolongations in the P-P interval (without relation to respiration). Approximately half of all newborns exhibit sinus pauses (Southall et al) and this is considered a normal finding. Sinus pause occurs in about 10% of teenagers. It is considered a normal finding if it occurs a few times a day. The pause shall not exceed 2 seconds. If the pause exceeds 2 seconds (>2.5 seconds are defined as sinus arrest), or if pauses are frequent or consecutive, this may be explained by sinus node dysfunction, hypersensitive carotid reflex or overactive vagus nerve (Figure 4).
Children with sensitive carotid reflex or overactive vagus nerve may have many sinus arrest/sinus pauses. Those with overactive vagus nerve may experience sinus pause/sinus arrest during sleep, during defecation, food intake and other situations of excessive vagus strain.
Ectopic atrial rhythm
Ectopic atrial rhythm occurs frequently in children. This rhythm is characterized by abnormal P-waves in lead II, notably retrograde (negative) P-waves. Healthy children monitored with Holter ECG often exhibit periods of ectopic atrial rhythm. Approximately 20% of all children exhibit an ectopic supraventricular rhythm (Goodacre, BMJ, 2002); these episodes rarely last more than 1 minute and are more common during sleep.
Ectopic atrial rhythm with varying P-wave morphology indicates that there are multiple ectopic foci. Such arrhythmias are referred to as wandering atrial pacemaker if the ventricular rate is below 100 beats/min, and multifocal atrial tachycardia (MAT) if the ventricular rate is ≥100 beats/min.
Other tachyarrhythmias
Tachyarrhythmias in pediatric patients are diagnosed in the same way as in adults (see Diagnosis and Management of Tachyarrhythmias/Tachycardia). AVNRT and AVRT are, second to sinus tachycardia, the most common causes of narrow complexes tachycardia (QRS duration <0.12 sec). Atrial fibrillation and atrial flutter are rare and indicate structural heart disease (atrial fibrillation and flutter are also common post-cardiac surgery).
Junctional tachycardia (junctional ectopic tachycardia, JET) also occurs in children.
In total, approximately 90% of all tachyarrhythmias in pediatric patients are supraventricular. The remaining 10% are ventricular and, as in adults, are more serious. Approximately half of the patients with recurring tachyarrhythmias are shown to have a structurally normal heart. Among the rest, structural heart disease and Wolff-Parkinson-White syndrome (pre-excitation) are the most common causes.
Tachyarrhythmia with a wide QRS complex (QRS duration ≥0.12 sec) should be regarded as ventricular tachycardia until proven otherwise. However, as for adults, tachyarrhythmias with wide QRS complexes can be supraventricular, with the wide QRS complex being explained by e.g bundle branch block, hyperkalemia or aberrant conduction. Methods for distinguishing ventricular tachycardia and supraventricular tachycardia with wide QRS are the same as for adults.
Ventricular tachycardia in children can be either monomorphic (e.g cardiomyopathy, congenital heart disease, etc.) or polymorphic (e.g long QT syndrome [LQTS], familial catecholaminergic polymorphic ventricular tachycardia and Brugada syndrome).
It should be noted that tachyarrhythmias in children can display very high ventricular rates. In neonates and infants, ventricular rate up to 330 beats/min is possible and >200 beats/min is common. Young children and adolescents usually display frequencies around 150-250 beats/min. Pediatric patients, similar to adults, can endure tachyarrhythmias for long periods but decompensation can occur without warning, particularly in patients with structural heart disease.
Administration of adenosine in pediatric patients
Dosing: intravenous or intraosseous adenosine 0.1 mg/kg, given as a rapid bolus (maximum of 6 mg). If unsuccessful, a second dose of 0.2 mg/kg rapid bolus (maximum of 12mg) can be given. Each bolus is immediately followed by a NS bolus. Side effects include flushing, chest discomfort, transient asystole or bradycardia. A halved dose should be used for patients taking dipyridamole or carbamazepine, which both potentiate the effects of adenosine. Halved dose is also given to heart transplant patients and in central line use.
Adenosine is the primary choice to treat stable narrow-complex tachycardia. When given as a rapid bolus, adenosine slows conduction in the heart, particularly in the AV node. This may terminate reentry pathways and restore sinus rhythm.
Beta-blockers and verapamil should not be used to treat tachyarrhythmias; beta-blockers lack anti-arrhythmic effect and verapamil may exacerbate tachyarrhythmias using accessory pathways (i.e WPW syndrome).
Vagal maneuvers may have the same effect as adenosine and could be attempted before administering adenosine. There are multiple vagal maneuvers (carotid massage, Valsalva maneuver, cold water in the face, etc).
Adenosine should only be administered by experienced personnel, with readiness for cardiopulmonary resuscitation. Adenosine is administered under continuous ECG monitoring.
Synchronized cardioversion
Acute cardioversion is performed in impending or manifest circulatory collapse. Consciousness is a contraindication for cardioversion. Anesthesia may be necessary to cardiovert.
Sinus bradycardia
Sinus bradycardia implies that criteria for sinus rhythm are fulfilled but the heart rate is below the lower normal limit (age-related). Bradycardia is generally more alarming than tachycardia. The causes of sinus bradycardia are as follows: hypoxia, hypothermia, hypothyroidism, AV block, increased intracranial pressure, LQTS, meningitis, acidosis, and sepsis. Stable patients with sinus bradycardia should initially be examined with Holter ECG.
Premature supraventricular and ventricular beats
Premature supraventricular beats occur already from birth. Supraventricular beats are more common than ventricular beats in the first year of life. Most healthy children exhibit only one or a few premature beats per hour and they usually disappear during physical activity (indicating that they are benign).
Premature ventricular beats are seen in 30% of healthy children. Generally, these premature beats are unifocal (i.e all beats display identical QRS appearance). Consecutive ventricular beats and multifocal ventricular beats (i.e the beats display varying QRS appearance) are less common. Premature beats in bigemini, trigemini, and quadrigemini also occur. In the vast majority of healthy people, the number of ventricular premature beats is <50 beats per day. These beats should disappear during physical exercise.
P-wave
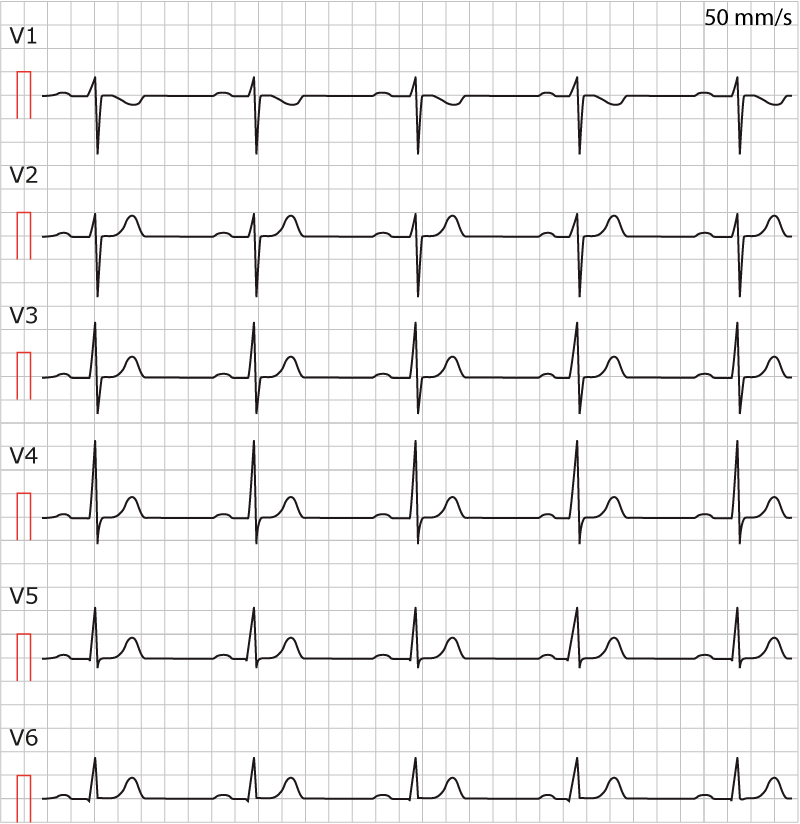
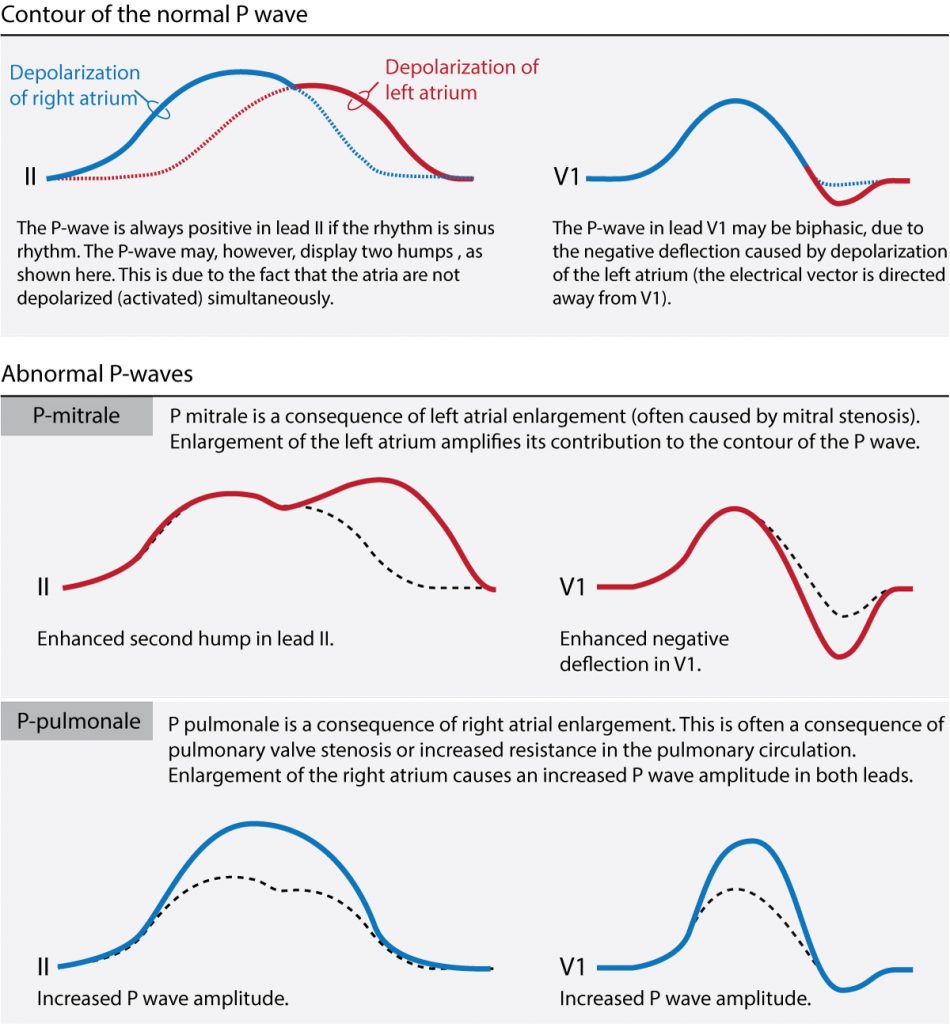
The appearance, amplitude, and duration of the P-wave change very little during the course of life. Reference values for adults and children are virtually identical. The amplitude of the P wave should be <2.5 mm (98th percentile) in lead II and <1.5 mm in lead V1.
Abnormal P waves: atrial abnormality
P-pulmonale
If the P-wave amplitude exceeds 2.5 mm in lead II or 1.5 mm in lead V1, right atrial enlargement should be suspected. This finding is referred to as P-pulmonale.
P-mitrale
Left atrial enlargement is suspected if the duration of the P-wave is prolonged, especially if the P-wave is two-humped in lead II and clearly biphasic in lead V1. See
P-mitrale and P-pulmonale are illustrated in Figure X.
4. PR interval
The mean PR interval at birth is 107 ms (Davignon et al). Due to changes in sympathetic and parasympathetic tone, the PR interval decreases to 98 ms (mean) by the age of 1 month. Subsequent atrial growth and changes in autonomic balance result in a successive increase in PR interval after 1 month of age.
Pre-excitation and atrioventricular (AV) block
Assessment of the PR interval is the same in pediatric and adult patients. Short PR interval (i.e. PR interval shorter than 2nd percentile, see Normal values for Pediatric ECG) suggests pre-excitation. The principles of pre-excitation in children are the same as for adults. For details, refer to Pre-excitation and Wolff-Parkinson-White Syndrome.
Prolonged PR interval suggests AV block. Long PR intervals during sleep are, however, normal; the PR interval may exceed 200 ms during sleep, which is explained by the high vagal tone in children. Thus, first-degree AV block is normal in pediatric patients during sleep. Single episodes of first-degree AV block during the day are also considered normal in children. However, frequent and recurring episodes of first-degree AV block are pathological. There are multiple causes of first-degree AV block in children, e.g pericarditis, myocarditis, perimyocarditis, Ebstein’s anomaly, endocardial cushion defect (ESD), atrial septal defect (ASD), digoxin effect and hyperkalemia.
Second-degree AV block type 1 (Wenckebach block) is considered a normal finding during sleep and as single episodes during the day. More frequent episodes of second-degree AV block suggests underlying disease.
Third-degree (complete) AV block is rare and mostly a sign of significant heart disease. Congenital (structural) heart disease is one of the most common causes of third-degree AV block in children. Postnatal onset of third-degree AV block should also raise suspicion of autoimmune AV block. Maternal anti-Ro-SSA and anti-La-SSB autoantibodies (common in connective tissue diseases) can be transferred to the fetus via the placenta. These autoantibodies target the electrical conduction system, which may result in third-degree AV block. Other common causes of third-degree AV-block are myocarditis, cardiac surgery involving the lower region of the atria, the atrial septum, or upper ventricular septum. Mortality in congenital third-degree AV block is high in neonates and infants.
Complete AV block may be preceded by first- and second-degree AV block, which is why it is recommended that repeated ECG tracings are acquired in patients with first- or second-degree AV-block. An ECG should also be obtained on the mother to a child born with AV block. Analysis of anti-Ro-SSA and anti-La-SSB is also indicated. Neonates with second- or third-degree AV block should undergo thorough examinations, including imaging modalities.
ECG criteria for AV block in children is identical to criteria in adults, with the only exception being the upper normal limit for PR interval (for normal values, please refer to Normal values for Pediatric ECG).
Causes of short PR interval in pediatric patients
- Pre-excitation (Wolff-Parkinson-White syndrome)
- Pompe Disease
- Fabry Disease
- Ectopic atrial rhythm with a focus in proximity to the AV node
Ectopic atrial rhythms originating near the AV node may result in a short PR interval, simply because the distance between the AV node and the ectopic focus is short.
Note that in some cases ectopic atrial beats, or atrial rhythms, may display a longer PR interval, as compared with sinus beats, which is explained by the fact that the AV system may become exhausted during rapid atrial depolarizations.
Accessory pathways and pre-excitation
The atrioventricular (AV) node and the bundle of His are normally the only communications between the atria and the ventricles. The atrial impulse must pass through the AV node, which delays the impulse due to its slow conduction, before the impulse reaches the ventricles. Some individuals, however, possess an additional pathway between the atria and the ventricles. Such pathways can transmit the atrial impulse to the ventricles directly, without passing the AV system. These pathways are termed accessory pathways (or bundle of Kent). Accessory pathways are embryological remnants. Such pathways may be able to conduct the impulse from the atria to the ventricles (antegrade direction), from the ventricles to the atrial (retrograde direction) or both.
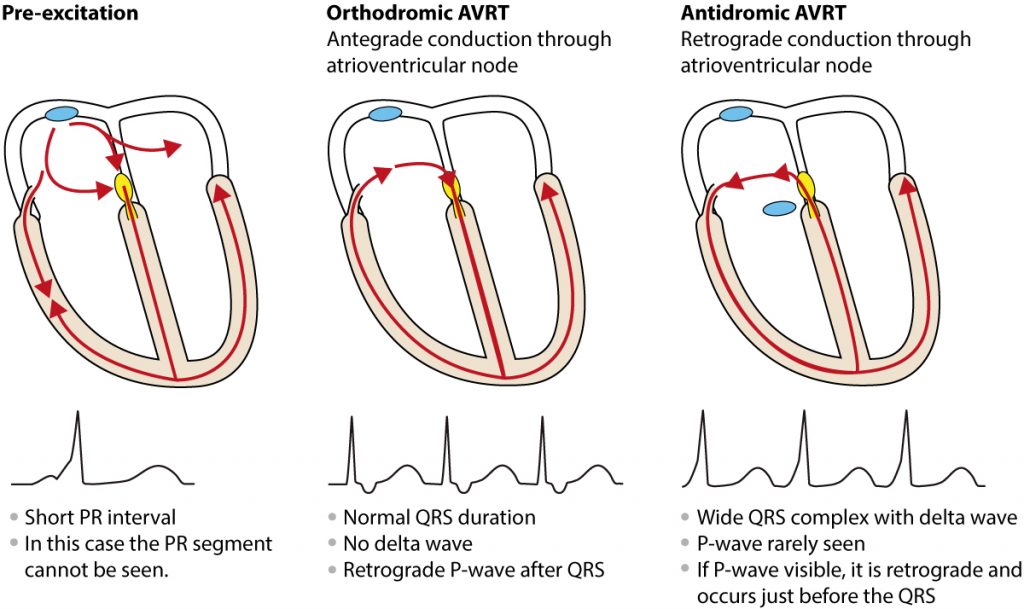
Accessory pathways are capable of rapid conduction, which means that any impulse reaching the accessory pathways may travel directly to the ventricles without any delay. Hence, the ventricles may be excited (depolarized) earlier than expected, which is referred to as pre-excitation. This manifests with three features on the ECG and the combination of these features are unique to pre-excitation:
- Short PR interval: The PR interval is shorter than the age-specific lower normal limit.
- Delta wave: depolarization of ventricular myocardium will start where the accessory pathway inserts into the ventricle, and the impulse will spread slowly because it propagates outside of the conduction system. This is reflected on the ECG as a slow start of the QRS complex and this part of the QRS complex is referred to as a delta wave.
- Prolonged QRS duration: Because the delta wave is included in the QRS duration, the total QRS duration will be prolonged.
As in adults, pediatric patients with accessory pathways only exhibit pre-excitation when impulses are actually conducted over the accessory pathway. In the majority of patients, conduction over the accessory pathway is intermittent, meaning that pre-excitation may not be seen at all times.
Wolff-Parkinson-White syndrome
Patients with evidence of pre-excitation who also have recurring tachyarrhythmias are said to have Wolff-Parkinson-White syndrome.
The tachyarrhythmia specific to WPW syndrome is atrioventricular reentrant tachycardia (AVRT). This arrhythmia is caused by a macroscopic re-entry circuit that involves the atria, atrioventricular node, accessory pathway, and the ventricles. In most cases, the re-entry is induced by a premature atrial beat.
There are two types of AVRT in children: orthodromic and antidromic. In orthodromic AVRT the re-entry impulse circulates in antegrade direction through the atrioventricular node. In antidromic AVRT the impulse travels in retrograde direction through the atrioventricular node.
Conduction via the accessory pathway may be present already at birth. Conduction is typically intermittent, meaning that delta waves are not always visible. Moreover, some accessory pathways are only capable of conducting from the ventricles to the atria; these patients show no evidence of pre-excitation on resting ECG but may experience tachyarrhythmias. This type of WPW is referred to as concealed WPW syndrome.
In addition to the classical ECG findings in pre-excitation, the following findings can also be seen during pre-excitation:
- Absence of septal q-waves in leads V5 and V6.
- Left axis deviation
These two findings may be visible in borderline cases (e.g. if the PR interval is borderline significant). For details see Perry et al.
Perry et al: Clues to the electrocardiographic diagnosis of subtle Wolff-Parkinson-White syndrome in children. J Pediatr 117:871, 1990.
The prevalence of WPW syndrome among pediatric patients is approximately 0.1% to 0.2%. Prevalence is higher among children with congenital heart disease. It is recommended that echocardiography be performed in children with evidence of pre-excitation.
Note that digoxin and verapamil, which reduce the refractory period of the accessory pathway, must not be administered to patients with evidence of pre-excitation, since these drugs may increase conduction via the accessory pathway. Moreover, adenosine is contraindicated in patients with irregular wide-complex tachyarrhythmias; these arrhythmias may be caused by pre-excited atrial fibrillation and adenosine can result in a complete AV block, which subsequently results in ventricular fibrillation (for details, refer to Pre-excitation (Wolff-Parkinson-White syndrome).
Causes of varying PR interval
- Wandering atrial pacemaker (WAP): caused by multiple ectopic atrial foci firing, which results in P-waves with varying morphology.
- Multifocal atrial tachycardia (MAT): Similar to WAP, but causing tachycardia.
- AV block II type 1 (Wenckebach block).
The QRS complex
Electrical axis (heart axis)
Most newborns have an electrical axis greater than 135° (98% confidence interval 58° to 168°). After birth, the electrical axis gradually normalizes (as the left ventricle becomes larger), which means that it falls between -30 and +90°. The causes of axis deviation are discussed below.
QRS duration
QRS duration should be measured in the lead with the longest QRS duration (which is usually a lead with visible Q-wave). At birth, the QRS time is <80 ms and then it gradually increases. The short QRS time in pediatric patients is due to the relatively small mass of the myocardium. During development, the ventricular mass increases, and the QRS duration becomes longer. As for adults, prolonged QRS duration means that depolarization of the ventricles is abnormally slow. This can be explained by the following conditions:
- Bundle branch block (RBBB, LBBB)
- Nonspecific intraventricular conduction delay
- Pre-excitation
- Hyperkalemia
- Ventricular rhythms
- Drug side effects
A diagnosis of bundle branch block (right or left bundle branch block) is made if the QRS duration is 20% above the age-specific upper normal limit (98th percentile). If the QRS duration is longer than the 98th percentile, but not by 20%, then a diagnosis of incomplete bundle branch block is made. If the QRS duration is prolonged but the QRS morphology is not compatible with either right or left bundle branch block, then a diagnosis of nonspecific intraventricular conduction delay can be made, provided that other causes of long QRS duration have been excluded.
Since bundle branch blocks and fascicular blocks are extremely rare among healthy children, the presence of these defects should lead to a thorough cardiological investigation. Several congenital heart diseases can lead to bundle branch blocks and fascicular blocks. In the setting of Ebstein’s anomaly, right bundle branch block is typically accompanied by prolonged PR interval.
R-wave and S-wave
At birth, the R-wave amplitude in V1-V3 is high, which is explained by the large right ventricle. The amplitude of the R-waves in V1-V3 decreases gradually with age, while the amplitudes of R-waves in V4-V6 increase as the left ventricle becomes larger. At 6 months of age, R-waves are usually tallest in V3-V4. S-waves display the opposite development (i.e. the depth gradually decreases in V4-V6 and increases in V1-V3). Note that the S-waves at birth tend to be deep in lead V1-V2, despite the tall R-waves (this is not seen among adults). Similarly, the S-waves are pronounced in V4-V6, where they can be 10 mm deep.
The amplitude of the R-waves and the S-waves should be assessed. Additionally, the R/S ratio, which is the amplitude of the R-wave divided by the amplitude of the S-wave, can be calculated. At birth, the R/S ratio in lead V1 is greater than 1 (which simply means that the R-wave is greater than the S-wave). The R/S ratio in V1 should be >1 until the age of 3 years. It is rare for patients with structurally normal hearts to have R/S ratio >1 in V1 after 5 years of age.
Notched R-waves in lead V1 are common. Such notches are usually seen after 1 month of age (Chia et al).
Chia et al: Cardiac time intervals of normal fetuses using noninvasive fetal electrocardiography. Prenat Diagn 25:546, 2005).
Causes of high R-wave amplitude (high voltage)
- Left ventricular hypertrophy (V4–V6)
- Right ventricular hypertrophy (V1–V3)
- Pre-excitation
- Right bundle branch block (V1–V3)
- Left bundle branch block (V5–V6)
Causes of low R-wave amplitude (low voltage)
- Hypothyreosis
- Pericardial fluid, tamponade
- Myocarditis
- Normal variant
Q-waves
Newborns normally display Q-waves in V5-V6 (septal q-waves). The amplitude of these Q-waves varies with age. Older children also display Q-waves in inferior leads (II, III, aVF). Across the age span, normal Q-waves are <30 ms in duration, and amplitudes rarely exceed 5 mm (although normal Q-waves may be up to 10 mm, especially in lead III).
Q-waves in V1-V3 (qR complexes) are always pathological. qR complexes in V1-V3 suggest right ventricular hypertrophy. The absence of septal q-waves in V5-V6 suggests left bundle branch block (provided the QRS duration is prolonged). Abnormally deep Q-waves suggests hypertrophy. As in adults, abnormal Q-waves can be caused by myocardial infarction, although this is very rare in children unless they have familial hypercholesterolemia or Kawasaki disease.
The presence of Q-waves in lead aVL and I is considered pathological. If there are no Q-waves in inferior leads, and instead large (≥ 3 mm deep and ≥30 ms wide) Q-waves in aVL and I, then coronary artery anomaly should be suspected.
Right ventricular hypertrophy
ECG has low sensitivity (approximately 20%), but high specificity (approximately 85%) for hypertrophy in pediatric patients (Rivenes et al, Am Heart J, 2003). This implies that the ECG detects 20% of cases with hypertrophy, and 85% of those who meet ECG criteria for hypertrophy actually have hypertrophy. Below follows a list of ECG changes seen in right ventricular hypertrophy.
- Right axis deviation (age-related cut-offs).
- The presence of Q-waves in V1 (qR complex) strongly suggests right ventricular hypertrophy.
- In severe right ventricular hypertrophy, the R-waves in V1 and V4R are higher than normal. The S-waves in V5-V6 are deeper than normal.
- The presence of rSR’ complexes in V1 suggests right ventricular hypertrophy (QRS duration should be normal, otherwise right bundle branch block should be suspected).
- S-wave in V6 deeper than 98th percentile.
- R/S ratio in V1 above than 98th percentile.
- R/S ratio in V6 below than 2nd percentile.
- From 7 days to 7 years of age, the T-wave in V1 and V4R is normally negative. If the T wave is positive in V1 and V4R during this period, right ventricular hypertrophy should be suspected.
- P-pulmonale suggests right ventricular hypertrophy.
Left ventricular hypertrophy
- Left axis deviation (age-specific cut-offs).
- High R-waves in V5 and V6.
- Deep S-waves in V1 and V4R.
- R/S ratio in V1 and V2 is smaller than normal.
- R/S ratio in V5 and V6 is greater than normal.
- Abnormally large Q-waves in V5-V6.
- ST-depression and T-wave inversion in V5-V6.
Biventricular hypertrophy
If criteria for both left and right ventricular hypertrophy coexist, then biventricular hypertrophy should be suspected.
Hypertrophic obstructive cardiomyopathy (HOCM)
Hypertrophic cardiomyopathy (HCM) is a genetically caused cardiomyopathy characterized by hypertrophy in the absence of hypertension, aortic stenosis, or other causes of increased left ventricular filling pressure. In approximately 70% of cases, hypertrophy causes obstruction of the left ventricular outflow tract (LVOT). The combination of hypertrophy and LVOT obstruction is referred to as hypertrophic obstructive cardiomyopathy (HOCM).
HCM/HOCM can manifest already in childhood. Dyspnea, chest pain, palpitations, pre-syncope/syncope are common symptoms. These patients have an increased risk of sudden cardiac death, heart failure, and atrial fibrillation. ECG is a relatively sensitive instrument for the detection of HCM/HOCM, since only 5-10% of patients have normal ECG at onset (Veselka et al).
Veselka et al: Hypertrophic obstructive cardiomyopathy, The Lancet (2017)
ECG characteristics of HCM/HOCM
- Signs of left ventricular hypertrophy, as well as secondary ST-T changes.
- P-mitrale
- Prominent Q-waves in V4, V5, V6, I, aVL, aVF, II and III. These Q-waves are mostly deeper than 3 mm and wider than 40 ms.
- Repolarization (ST-T) abnormalities.
- Left axis deviation.
- Giant T-wave inversions in the precordial leads. This suggests apical hypertrophy.
- Holter ECG can reveal supraventricular arrhythmias (especially atrial fibrillation), ventricular rhythms, and ventricular tachycardia. Supraventricular and ventricular extrasystoles are also common.
- Pre-excitation is more common among patients with HCM/HOCM, but likewise, the PR interval may be prolonged.
- Conduction defects are relatively common in HCM/HOCM.
The ST-segment
The ST-segment is normally isoelectric and it continues gradually into the T-wave. Among healthy children, ST-depressions <0.5 mm are sometimes seen in the limb leads. Healthy children rarely display ST-depressions in the chest (precordial) leads. As in adults, ST-depression with horizontal or downsloping ST-segment is more alarming than upward sloping ST depressions. Upward sloping ST-depressions are normal at high heart rates.
ST-elevations may occur in children, especially adolescents. ST-elevations are most common in precordial leads (V2-V6) and may reach 2 mm (measured in the J point). The most common causes of ST-segment elevations are as follows:
Normal ST-segment elevation and early repolarization manifest in the same way in children and adults.
Acute myocardial infarction is rare in children. Ischemic ST-elevations in children are similar to those seen in adults. However, perimyocarditis (myocarditis) is the most common cause of chest pain with ST elevations among children. Hyperkalemia, pneumothorax, as well as coronary artery anomaly can also cause ST elevations.
T-wave
At birth, the T-waves in lead V3R and V1 are positive, but within 7 days they become inverted. In most cases, the T-waves are also inverted in V2 and V3. These T-wave inversions persist until 10 years of age (sometimes up to 15 years). Thus, T-wave inversions in leads V3R, V1, V2, V3 are normal between 7 days and 10 to 15 years of age. The absence of T-wave inversions in these leads should lead to suspicion of right ventricular hypertrophy. After the age of 10 to 15 years, the T-waves gradually become positive (this starts in lead V3 and gradually moves towards lead V3R). Some children continue to display a negative T wave in V1 and this is a normal finding (the T-wave inversion is concordant with the QRS complex, which is also negative in lead V1). See Figure 7.
Juvenile T-wave pattern is diagnosed if the T-waves are not normalized after puberty (i.e. continued T wave inversion in leads V1-V3).
Global T-wave inversion exists when T-waves are inverted in all precordial leads, without evidence of heart disease, in adulthood and beyond.
Causes of high, flat and negative T waves in children are the same as in adults.
U-wave
Assessment of the U-wave in children does not differ from that in adults. It appears occasionally, mostly during slow heart rate, in leads V2-V4.
QT interval (QTc)
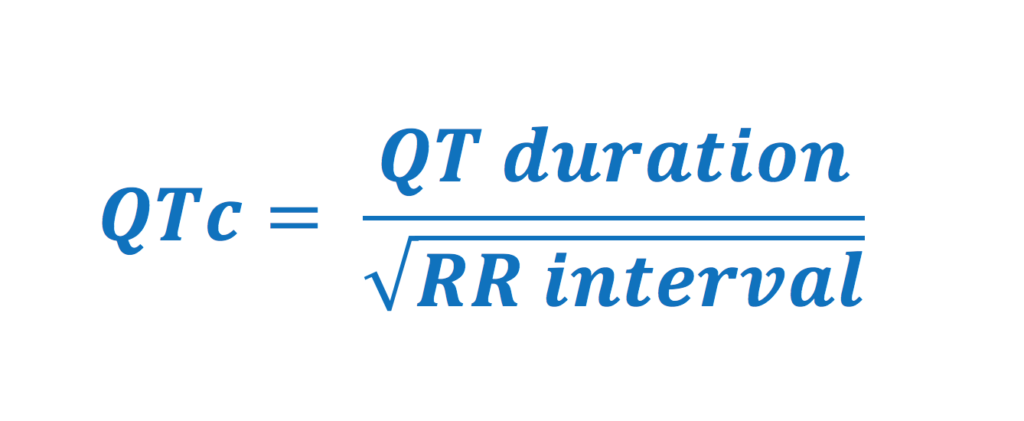
The QT interval reflects the total duration for ventricular de- and repolarization. This corresponds to the interval from the beginning of the QRS complex to the end of the T wave. Since the QT interval is inversely related to heart rate (QT interval becomes shorter at higher heart rates), the QT interval must be corrected for heart rate. This is called corrected QT (QTc) interval.
Assessment of QTc interval is very important since prolonged QTc interval increases the risk of malignant ventricular arrhythmias and sudden cardiac death (Long QT syndrome, LQTS). The automatically calculated QTc interval should always be checked by manual calculation (Miller et al: Diagnostic accuracy of screening electrocardiograms in long QT syndrome I. Pediatrics 108:8, 2001). Manual measurement of QT interval should be done in the precordial leads. The interval is measured from the earliest QRS deflection (in any lead) to the end of the T-wave (in any lead). This means that the start of the interval can be defined in e.g. lead V2 and the end defined in lead V5. U-waves should not be included in the measurement. Once the QT interval is measured, it is corrected for heart rate using Bazzet’s formula:
Causes of prolonged QTc interval
- Hypokalemia
- Hypocalcemia
- Hypothermia
- Drug side effects
- Cerebrovascular insult
- Ketogenic diet
- Acute weight loss
- LQTS
- Pericarditis, myocarditis, perimyocarditis
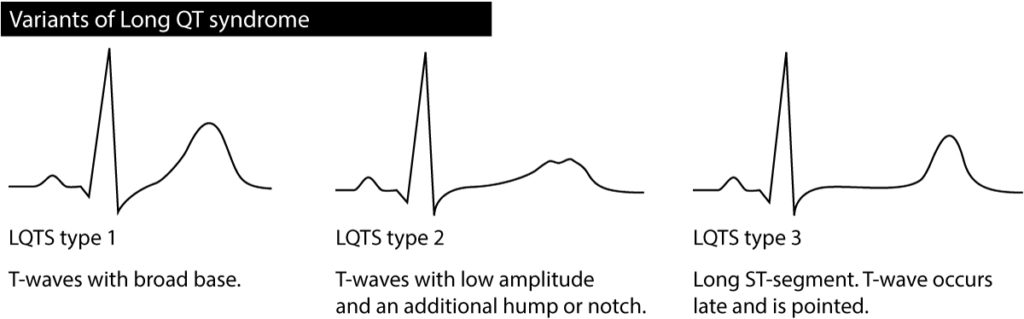
The prevalence of LQTS is 0.05% among children. For details, please refer to Long QT syndrome (LQTS). LQTS may cause one or several of the following ECG changes:
- Long QTc interval
- T-wave alternans: the amplitude of the T-wave varies from beat to beat.
- Abnormal T-wave morphology.
- Bradycardia.
- Torsade de pointes ventricular tachycardia.
Note that children with LQTS may occasionally show a normal QTc interval. As a rule, the longer the QTc interval, the more dangerous the condition. At QTc interval 500 ms there is a significant risk of ventricular arrhythmias and at 600 ms there is a very high risk.
Mortality in LQTS is very high if the condition is left untreated. 5-year mortality is 10% (Schwartz PJ et al). The genetic cause and treatment of LQTS have been discussed previously. LQTS is usually hereditary but may occur as de novo mutation. Some mutations display low penetration, which is why parents may carry the mutation with normal QTc interval.
It should also be noted that all children with prolonged QTc interval on one ECG tracing do not necessarily have LQTS. The management of pediatric patients with prolonged QTc interval is discussed in detail in the European guidelines available here.
Schwartz PJ et al, in Zipes DP et al: Cardiac electrophysiology: from cell to bedside, 3rd edn. Philadelphia: WB Saunders, 2000:597-615
Differential diagnoses to short QTc interval
Short QT (QTc) interval is associated with an increased risk of ventricular tachycardia. There are three causes of short QTc interval:
- Hypercalcemia
- Digoxin
- Congenital short QTc interval (Short QT syndrome), which is very rare.
Figure 9. Short QT-syndrome (SQTS). ECG recorded in 16 years old female. The QT-duration is 250 ms.