Electrolyte imbalance and cardiac arrest
Significant electrolyte imbalances can precipitate cardiac arrest and are potentially reversible etiologies when promptly and appropriately addressed. Both venous and arterial blood gases can be utilized for the analysis of electrolyte levels. Electrocardiography (ECG) serves as a valuable tool for detecting and assessing the severity of electrolyte disturbances, particularly before laboratory results are available. Notably:
- Both hyperkalemia and hypokalemia can induce life-threatening arrhythmias and cardiac arrest, with hyperkalemia being the most prevalent electrolyte disturbance observed in cardiac arrest scenarios.
- Hypocalcemia, although capable of causing cardiac arrest, is an infrequent occurrence.
- Hypercalcemia, hyponatremia, hypernatremia, hypomagnesemia, and hypermagnesemia are exceedingly rare precipitants of cardiac arrest.
Sodium imbalance
Neither hyponatremia nor hypernatremia typically cause discernible ECG changes.
Hyponatremia
Effective management of hyponatremia requires careful identification of its etiology, severity (Table 2), and temporal onset. Distinguishing between acute and chronic hyponatremia, based on the rapidity of onset, is of paramount importance. The primary concern in correcting hyponatremia is the prevention of osmotic demyelination syndrome (ODS), previously known as central pontine myelinolysis. Excessively rapid correction of sodium can result in catastrophic demyelination of pontine neurons.
- Acute Hyponatremia (<48 hours duration): Rapid correction is preferred. An increase of 1-2 mEq/L per hour for a total of 4-6 mEq/L in 24 hours may be targeted.
- Chronic Hyponatremia (>48 hours duration): Due to cellular adaptations, rapid correction carries the risk of inducing osmotic demyelination syndrome (ODS). It is therefore recommended to raise serum sodium by a maximum 8 mEq/L in the first 24 hours.
- Hyponatremia of unknown duration: These cases are managed as chronic hyponatremia.
| Degree of hyponatremia | P/S-Na+ | Common effects |
| Mild | >130-125 mmol/l | Cognitive disorders, vertigo, balance disorder. |
| Moderate | 115- 125 mmol/L | Headache, nausea, vomiting, muscle cramps, apathy, confusion, impaired reflexes. |
| Severe | <115 mmol/L | Seizures, coma, respiratory arrest, brainstem herniation and death. |
Hypernatremia
Hypernatremia does not cause cardiac arrest.
Calcium imbalance
Hypercalcemia
Definition: P/S-Ca2+ >2.6 mmol/L
In approximately 90% of cases, hypercalcemia is attributed to primary hyperparathyroidism or neoplastic etiologies. Other causes include immobilization, sarcoidosis, thyrotoxicosis, familial hypocalciuric hypercalcemia, Addison’s disease, renal insufficiency, therapeutic interventions with tamoxifen or lithium, thiazide administration, and over-supplementation of calcium and vitamin D.
ECG in hypercalcemia
- Typical ECG changes:
- Shortened QT interval.
- Attenuated T-wave amplitude.
- Prolonged QRS duration.
- AV-block (AV-block 1, AV-Block 2, AV-Block 3)
- Less frequent ECG changes:
- Increased QRS amplitude.
- Osborn waves.
- ST-elevation in V1-v2.
- Sinus node dysfunction (bradycardia).
- Ventricular tachycardia (VT), ventricular fibrillation (VF).
Clinical presentation
- Confusion
- Abdominal pain
- Hypotension
- Arrhythmias and ECG changes
- Cardiac arrest
Treatment
- Furosemide 1 mg/kg IV.
- Hydrocortisone 300 mg IV.
- Pamidronate 30-90 mg IV.
- Causal treatment of the underlying cause.
Hypocalcemi
Hypocalcemia may arise from various causes, including acute pancreatitis, alkalosis due to hyperventilation, rhabdomyolysis (particularly the initial phase), sepsis, malignancies with osteoblastic metastases, diminished calcium absorption and/or enhanced calcium excretion, chronic renal failure, pancreatic or bowel resections (leading to “short bowel syndrome”), parathyroid and thyroid surgeries, as well as medications and agents such as bisphosphonates, calcitonin, citrate (from transfusions), phenytoin, phosphate, and foscarnet, among others.
ECG in hypocalcemia
- Prolonged QT interval (torsades de pointes is unusual)
- Shortened QRS duration
- Less common ECG changes:
- AV block
- Sinus bradycardia
- SA block
- Ventricular fibrillation (VF)
Treatment
- Calcium chloride 10%, 10-40 ml IV.
- Magnesium sulfate 50%, 4-8 mmol IV in severe instances.
Potassium
The ECG is particularly useful in potassium disorders. The ECG can be used to approximate the severity of potassium imbalance.
Hyperkalemia
Causes of hyperkalemia:
- Kidney disease (acute renal failure, chronic renal failure, ESRD [end-stage renal disease]).
- NSAID (non-steroidal anti-inflammatory drugs): ibuprofen, naproxen, nabumetone, acetylsalicylic acid, etc.
- Hemolysis.
- Tumor light syndrome.
- Over-supplementation of potassium (medications or dietary).
- ACE (angiotensin-converting enzyme) inhibitors (enalapril, ramipril, etc).
- ARB (angiotensin receptor blockers) (losartan, candesartan, etc).
- ARNI (angiotensin II antagonists and neprilysin inhibitors) – sakubitril valsartan (Entresto) .
- MRA (mineralocorticoid receptor antagonists): spironolactine, eplerenone, finerenone, aldosterone, etc.
- Non-selective beta-blockers: propranolol, nadolol, timolol, etc.
- Rhabdomyolysis
- Acidosis
- Addison’s disease
- Insulin deficiency (diabetes, ketoacidosis)
- Potassium-sparing diuretics
- Digitalis intoxication
Within the myocardium, hyperkalemia results in prolonged impulse conduction. Clinically significant manifestations are evident when serum potassium concentrations exceed 7 mmol/L. It is postulated that hyperkalemia serves as a relatively frequent etiological factor for cardiac arrest, as suggested by studies from Wallmuller et al., Wang et al., and Saarinen et al. However, the proportion of cardiac arrests caused by hyperkalemia remains unknown and is likely to be low.
ECG in hyperkalemia
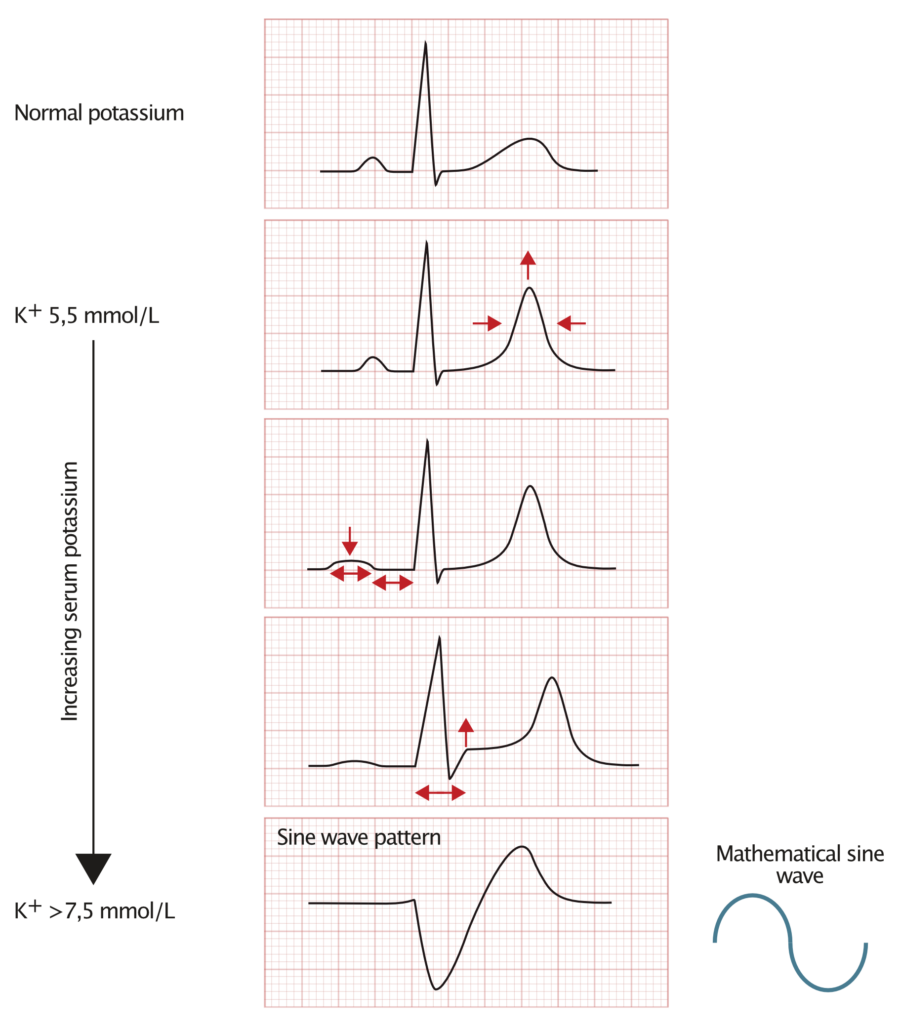
Mild hyperkalemia (P-Potassium 5.5—5.9 mmol/)
- Symmetrical, high, pointed and wide T-waves are the initial ECG changes.
- If the patient has left ventricular hypertrophy with secondary ST-T change since before, these can be “pseudonormalized”.
- T wave changes are best seen in the chest leads (typically V2-V5).
Moderate hyperkalemia (P-Potassium 6.0—6.4 mmol/)
- Diminished P wave amplitude.
- Prolonged PQ interval.
- Occasionally, SA block, AV block II, or AV block III occur.
- Patients with WPW syndrome may lose their delta wave because the accessory pathway functions poorly during hyperkalemia.
- Occasionally, ST elevations are seen in V1-V2.
Severe hyperkalemia (P-Potassium >6.5 mmol/L)
- Occasionally, ST elevation in V1-V2.
- Widening of the QRS complex.
- The broad QRS complex and T wave merge and the fused signal is called a sine wave. This indicates life-threatening potassium levels since it may progress rapidly to ventricular fibrillation or asystole.
Treatment of hyperkalemia
- In cases of severe hyperkalemia, administer 10 ml of either calcium gluconate or calcium chloride intravenously without delay.
- Initiate an infusion of insulin and glucose, comprising 25 g of glucose combined with 10 units of insulin.
- Continue with a subsequent infusion of 10% glucose solution over a 5-hour duration, delivering a total of 25 g of glucose.
- Consider the administration of salbutamol when appropriate.
- Hemodialysis remains the most efficacious intervention for hyperkalemia.
Hypokalemia
Causes of hypokalemia:
- Diarrhea and vomiting
- Diabetes insipidus
- Fluid loss from dialysis (hemodialysis, peritoneal dialysis)
- Alcoholism
- Malnutrition
- Primary or secondary hypoaldosteronism
- Excessive licorice intake
- High glucose infusion
- Use of diuretics
- Beta-adrenergic agonists (e.g., salbutamol)
- Theophylline
- Corticosteroid administration
- Cushing’s syndrome
- Laxatives
- Insulin therapy
- Hypomagnesemia
- Metabolic alkalosis
Complications of significant severity can manifest at levels as low as 3.0 mmol/L. Hypokalemia poses heightened risks in patients on digoxin therapy or those with structural heart abnormalities. Under these circumstances, hypokalemia may precipitate life-threatening ventricular arrhythmias.
Chronological ECG manifestations in response to decreasing potassium levels:
- The T wave demonstrates increased width and decreased amplitude. Severe hypokalemia can induce T-wave inversion.
- ST-segment depression.
- Prolongation of the PQ interval, accompanied by an augmented and broadened P-wave.
- Prolongation of the QT interval.
- The emergence of U-waves, which are most prominent in leads V2-V3. In cases of severe hypokalemia, the U wave amplitude might exceed that of the T wave.
- Potential progression to cardiac arrest, manifesting as pulseless electrical activity (PEA), ventricular fibrillation/pulseless ventricular tachycardia (VF/PVT), or asystole.
Hypokalemia can cause QT prolongation (i.e. cause acquired long QT syndrome), and thereby induce torsades de pointes (polymorphic ventricular tachycardia). Additionally, hypokalemia can precipitate ventricular tachycardia (VT) without concurrent QT prolongation. The risk of arrhythmias is further augmented in patients receiving digitalis therapy.
Treatment of hypokalemia
- Provide potassium with infusion 10 mmol/hr. Maximum infusion rate is 20 mmol/h.
- If the patient has threatening arrhythmias, 2 mmol/min is given for 10 min, followed by 10 mmol for 5-10 min. After that, the usual infusion is given. Take repeated measurements of S/P potassium to titrate the infusion speed.
- Give 4 ml magnesium sulfate 50% (8 mmol) diluted in 10 ml NaCl 0.9% over 20 minutes.
Magnesium imbalance
Hypermagnesemia
Definition of hypermagnesemia: >1.1 mmol/L Mg2+
Although rare, severe hypermagnesemia can cause atrioventricular and intraventricular conduction disorders that may culminate in AV Block III and asystole. The most common causes of hypermagnesemia are renal failure and iatrogenic hypermagnesemia.
Clinical features of hypermagnesemia
- Confusion, weakness, respiratory failure, AV block, cardiac stop.
- ECG changes in hypermagnesemia:
- Prolonged PR interval.
- Prolonged QT interval. However, hypermagnesemia does not cause torsade de pointes (TdP).
- Pointy and high T-waves.
- AV block.
- Cardiac arrest.
Treatment of hypermagnesemia
Treatment is indicated if P/S-Mg2+ >1.75 mmol/L.
- Injection calcium chloride 10%, 5-10 ml IV, repeat as necessary.
- Infusion NaCl 0.9% with added furosemide 1 mg/kg.
- Hemodialysis remains the most effective intervention for hypermagnesemia.
Hypomagnesemia
Definition of hypomagnesemia: S-Mg2+ <0.6 mmol/L
Hypomagnesemia may potentiate certain digitalis (digoxin) arrhythmias as well as potentiate, or possibly cause, supraventricular and ventricular arrhythmia.
- Causes of hypomagnesemia
- AlcoholismMalabsorptionGastrointestinal losses
- Polyuria
- Starvation
- Symptoms of hypomagnesemia
- Tremor
- Ataxia
- Nystagmus
- Seizures
- Hypomagnesemia can cause torsade de pointes (TdP)
- ECG changes
- Prolonged QRS duration.
- Torsade de pointes (TdP).
- Treatment of hypomagnesemia
- Severe hypomagnesemia: 2 g magnesium sulfate 50% (4 ml; 8 mmol) IV over 15 min.
- Torsade de pointes: 2 g magnesium sulfate 50% (4 ml; 8 mmol) IV over 1-2 min.
- In case of seizures: 2 g magnesium sulfate 50% (4 ml; 8 mmol) IV over 1-2 min.

