Cardiac arrest in hypothermia (accidental hypothermia)
Accidental hypothermia
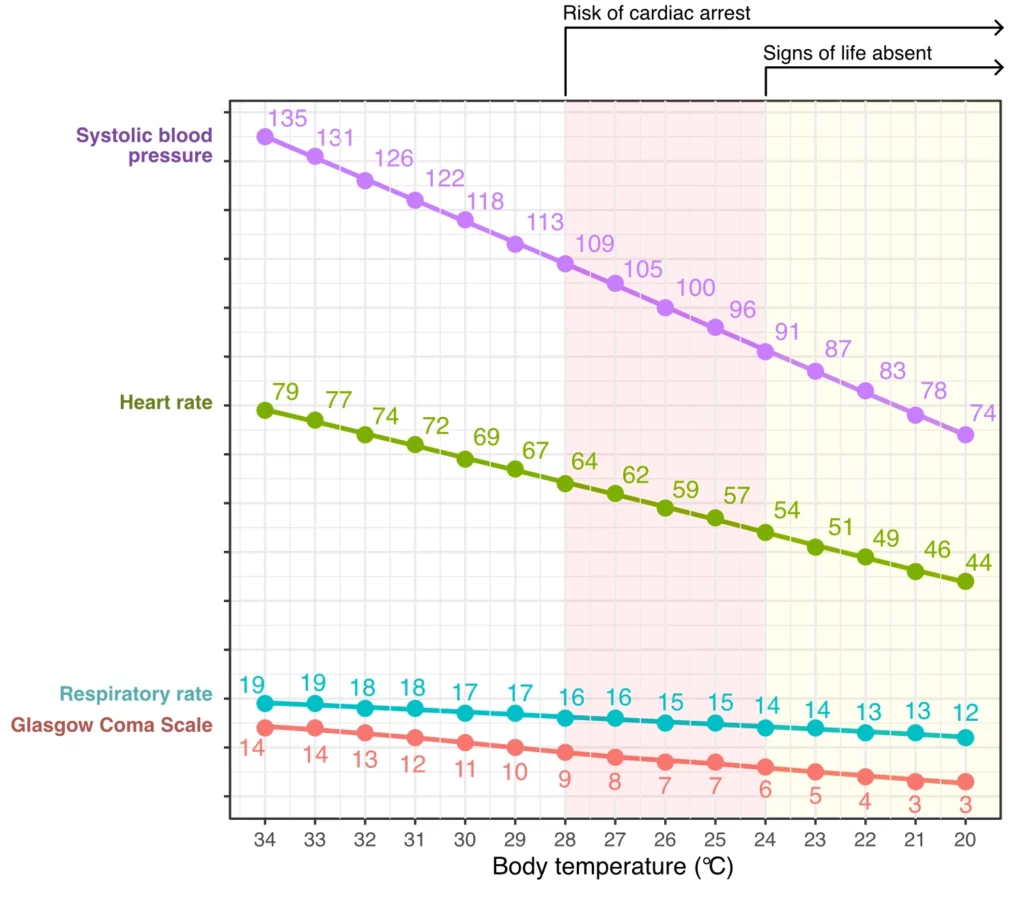
Accidental hypothermia is defined as an unintentional decrease in body temperature to below 35°C. The lowest recorded body temperatures from which patients have been successfully resuscitated are 11.8°C for accidental hypothermia and 4.2°C for medically induced hypothermia (Mroczek et al., Stephen et al.). Figure 1 illustrates the decline in cardiopulmonary function and consciousness with decreasing body temperature. There appears to be a linear relationship between body temperature and both cardiopulmonary function and alertness. Cardiac arrest is unlikely to occur when body temperature remains above 28° C (82.4° F), while temperatures below 24° C (75.2° F) are not compatible with signs of life (Frei et al.).
When hypothermia precedes cardiac arrest, the body has undergone cooling before circulatory cessation, enhancing the likelihood of survival. In such instances, favorable neurological outcomes are possible even with prolonged periods of no blood flow, due to the reduced metabolic rate that accompanies declining body temperature. For every 1°C reduction in body temperature, there is a 6% decrease in oxygen consumption (Wood et al.).
Evaluating the vitality of a hypothermic individual can be challenging, especially when discerning between hypothermic unresponsiveness and cardiac arrest. Frequently, overt signs of life are absent, and the patient’s coldness can mimic post-mortem conditions. Therefore, a meticulous assessment of vital signs is crucial.
Exceptionally high survival rates have been documented in cases of accidental hypothermia followed by cardiac arrest. For unwitnessed cardiac arrests under these conditions, the survival rate upon hospital arrival has been recorded at 27%, while for witnessed cardiac arrests, the survival rate stands at 73% (Podsiadlo et al.). A significant majority of these patients exhibit satisfactory neurological function upon discharge.
| Severity | Features | Body temperature (°C) |
|---|---|---|
| Mild hypothermia | Conscious with tremors | 32-35°C |
| Moderate hypothermia | Impaired consciousness, with or without shivering | 28-31°C |
| Severe hypothermia | Unconscious, with signs of life | <28 °C |
| Very severe hypothermia | No signs of life | <24 °C |
Actions in accidental hypothermia with cardiac arrest or cardiopulmonary depression
- Use HOPE Score to assess the prognosis.
- A long no-flow time can sometimes be compatible with survival with good neurological function, which is why CPR should be considered even with extended no-flow periods, in cases of unwitnessed cardiac arrests, as well as if the initial rhythm was asystole (Podsiadlo et al.).
- Assess life signs:
- Vital parameters.
- ECG.
- Capnometry (ETCO2).
- Echocardiography bedside.
- Heating is optimally achieved using extracorporeal membrane oxygenation (ECMO). In the absence of ECMO, both non-invasive and invasive rewarming techniques should be pursued.
- Heated intravenous fluids (crystalloids).
- Heated and moistened oxygen.
- Warm covers.
- Heat fan.
- Remove any cold or damp textiles.
- Administer cardiopulmonary resuscitation (CPR) following standard protocols, emphasizing concurrent rapid rewarming of the patient. Consider extracorporeal membrane oxygenation (ECMO) in unstable patients.
- The administration of medications (such as amiodarone and epinephrine) and defibrillation procedures should be deferred until the body temperature exceeds 30°C. This is due to the diminished efficacy of these interventions at low temperatures. Additionally, the return of spontaneous circulation (ROSC) is typically not sustained at temperatures below 30°C.
Concurrent Hypothermia and Asphyxia in Avalanche Incidents
Hypothermia coupled with asphyxia is commonly observed in victims of avalanche incidents. Typically, by the time emergency services arrive, the patient has succumbed due to asphyxiation. However, given the cooling effect associated with avalanches, it is advisable to attempt cardiopulmonary resuscitation (CPR) even in the context of extended no-flow periods. Initial management should encompass five rescue breaths, followed by the standard CPR for a minimum duration of 20 minutes before considering termination. In the context of avalanche incidents, CPR is advocated even if the individual has remained buried for up to 60 minutes.
References
DeBehnke DJ, Hilander SJ, Dobler DW, Wickman LL, Swart GL. The hemodynamic and arterial blood gas response to asphyxiation: a canine model of pulseless electrical activity. Resuscitation 1995;30:16975.
Safar P, Paradis NA, Weil MH. Asphyxial cardiac arrest. In: Paradis NA, Halperin HR, Kern KB, Wenzel V, Chamberlain DA, editors. Cardiac arrest—the science and practice of resuscitation medicine.
Kitamura T, Kiyohara K, Sakai T, et al. Epidemiology and outcome of adult out-of-hospital cardiac arrest of non-cardiac origin in Osaka: a population-based study. BMJ Open 2014;4:e006462.
Deasy C, Bray J, Smith K, et al. Hanging-associated out-of-hospital cardiac arrests in Melbourne, Australia. Emerg Med 2013;30:3842.
Luna GK, Pavlin EG, Kirkman T, Copass MK, Rice CL. Hemodynamic effects of external cardiac massage in trauma shock. J Trauma 1989;29:1430-3.
Jeffcoach DR, Gallegos JJ, Jesty SA, et al. Use of CPR in hemorrhagic shock, a dog model. J Trauma Acute Care Surg 2016;81:27-33.
Watts S, Smith JE, Gwyther R, Kirkman E. Closed chest compressions reduce survival in an animal model of hemorrhage-induced traumatic cardiac arrest. Resuscitation 2019;140: 37-42.
Endo A, Kojima M, Hong ZJ, Otomo Y, Coimbra R. Open-chest versus closed-chest cardiopulmonary resuscitation in trauma patients with signs of life upon hospital arrival: a retrospective multicenter study. Crit Care 2020;24:541.
Ebo DG, Clarke RC, Mertes PM, et al. Molecular mechanisms and pathophysiology of perioperative hypersensitivity and anaphylaxis: a narrative review. Br J Anaesth 2019;123:e3849.
Wallmuller C, Meron G, Kurkciyan I, et al. Causes of in-hospital cardiac arrest and influence on outcome. Resuscitation 2012;83:120611.
Wang CH, Huang CH, Chang WT, et al. The effects of calcium and sodium bicarbonate on severe hyperkalaemia during cardiopulmonary resuscitation: a retrospective cohort study of adult in-hospital cardiac arrest. Resuscitation 2016;98:10511.
Saarinen S, Nurmi J, Toivio T, et al. Does appropriate treatment of the primary underlying cause of PEA during resuscitation improve patients’ survival? Resuscitation 2012;83:81922.
Mroczek T, Gladki M, Skalski J. Successful resuscitation from accidental hypothermia of 11.8 degrees C: where is the lower bound for human beings? Eur J Cardiothorac Surg 2020;58:10912.
Stephen CR, Dent SJ, Hall KD, Smith WW. Physiologic reactions during profound hypothermia with cardioplegia. Anesthesiology 1961;22:87381.
Frei C, Darocha T, Debaty G, et al. Clinical characteristics and outcomes of witnessed hypothermic cardiac arrest: a systematic review on rescue collapse. Resuscitation 2019;137:418.
Wood S. Interactions between hypoxia and hypothermia. Annu Rev Physiol 1991;53:7185.
Podsiadlo P, Darocha T, Svendsen OS, et al. Outcomes of patients suffering unwitnessed hypothermic cardiac arrest rewarmed with extracorporeal life support: a systematic review. Artif Organs 2020.

