The physiology of cardiopulmonary resuscitation (CPR)

The forces that drive coronary and cerebral perfusion, and ventilation of the lungs during cardiopulmonary resuscitation (CPR) differ substantially from normal circumstances. The purpose of CPR is to create large variations in intrathoracic pressure by compressing, decompressing and ventilating. These maneuvers result in arterial blood flowing through the pulmonary, coronary and cerebral circulation, as well as allowing for gas exchange in the lungs. A large number of experimental and observational studies have been conducted to optimize the effectiveness of CPR. Yet, there are fundamental gaps in knowledge, with some of the most critical components of current guidelines being based on observational data (e.g compression rate and depth). With current strategies, compressions and ventilations can generate a cardiac output equivalent to 15-25% of normal output (Duggal et al). This, in conjunction with defibrillation, is sufficient to resuscitate 10-15% of out-of-hospital cardiac arrests (OHCA) and 30-40% of in-hospital cardiac arrests (IHCA; Jerkeman et al).
Current guidelines recommend a compression depth of 5–6 cm at a rate of 100–120 compressions per minute (Figure 1). These recommendations are based on observational data (Stiell et al, Idris et al, Duval et al). Randomized clinical trials are lacking.

Duval et al studied 3,643 cases of out-of-hospital cardiac arrest in the ROC PRIMED trial. These patients were enrolled in a randomized trial that evaluated the efficacy of a CPR adjunct and also recorded the compression rate and depth. They reported that the ideal combination was 107 compressions per minute with a depth of 4.7 cm. This combination was consistent across different ages, sexes, initial rhythms, and the use of CPR adjuncts.
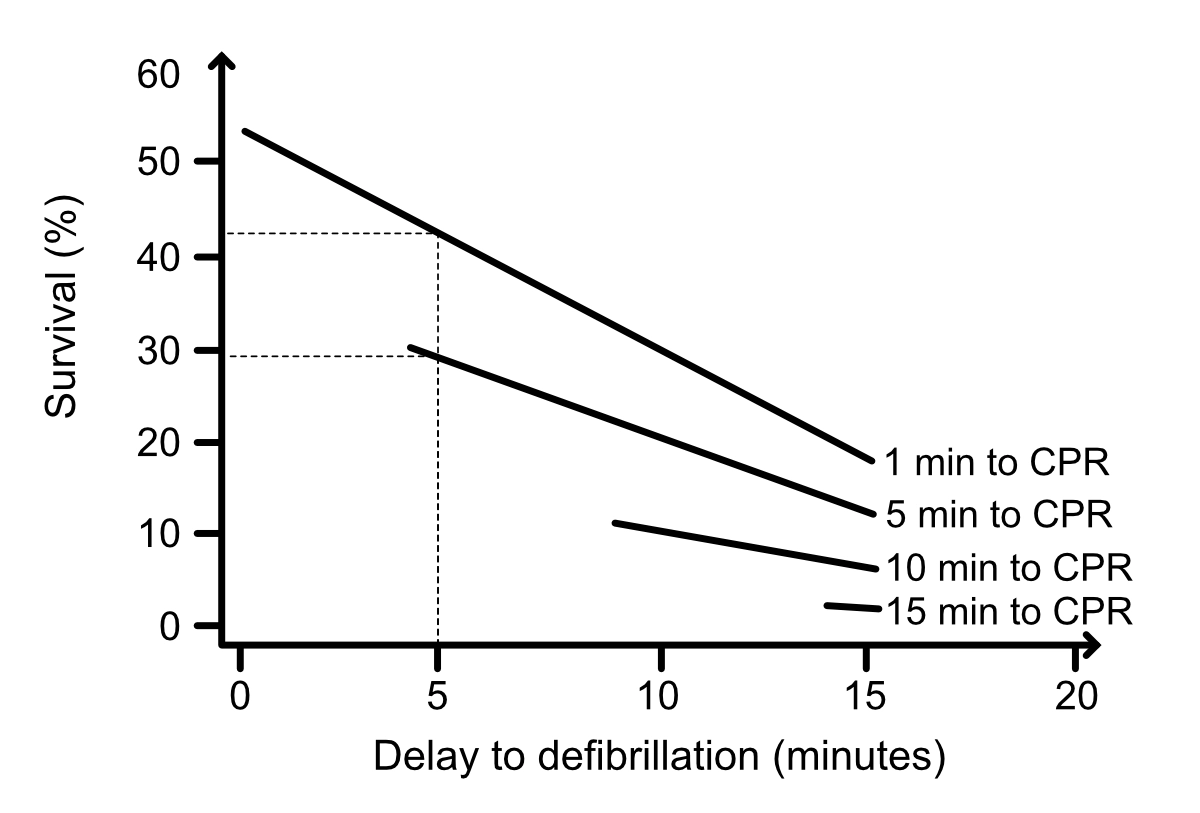
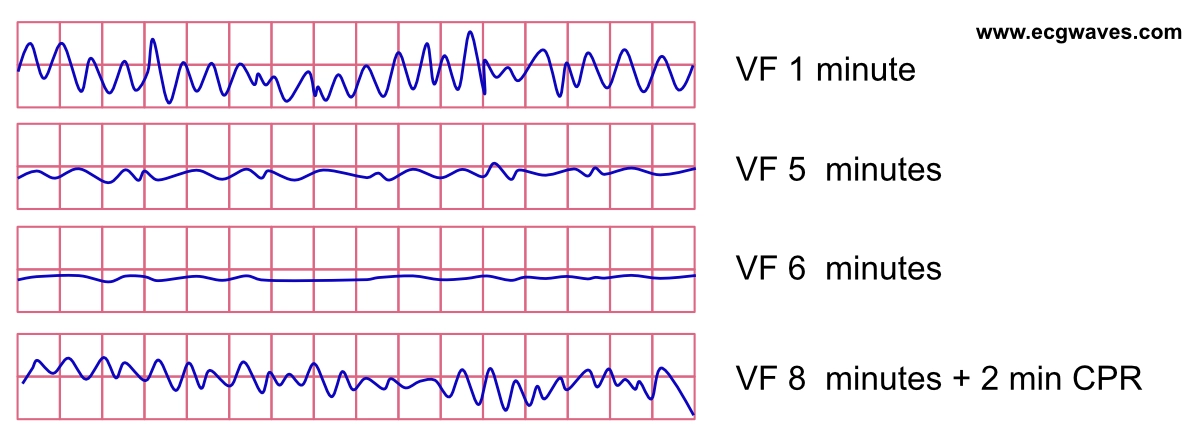
Defibrillation is the most important intervention if the rhythm is shockable (ventricular fibrillation [VF], pulseless ventricular tachycardia [VT]). The VF waveform is initially coarse (i.e fibrillatory waves have large amplitudes) but as the duration of VF is prolonged, the amplitude gradually diminishes and fine VF (small fibrillatory amplitudes) ultimately degenerate into asystole. The gradual progression from coarse VF to fine VF and finally asystole is the result of diminishing ATP concentration in the myocardium. ATP depletion results in cellular dysfunction and renders the defibrillation ineffective. The likelihood of successful defibrillation is high in coarse VF (the early phase), but diminishes rapidly as the waveform becomes finer (Figures 2, 3 and 4).

In circumstances with non-shockable rhythm or with prolonged periods of VF (fine VF resistant to defibrillations), the purpose of CPR is to induce myocardial electrical activity by generating adequate coronary perfusion pressure (CPP). Myocardial activity is necessary to salvage the brain, and is therefore of prime importance. This is achieved by performing effective chest compressions and decompressions that result in perfusion of cardiac, cerebral, and pulmonary tissue.
Chest compressions produce perfusion of vital organs by increasing the pressure in the atria, ventricles and large vessels. This results in blood being propelled forward (assuming that valvular function is normal). Unfortunately, the compressions also increase pressure in the thoracic veins (paravertebral veins, epidural veins) that drain the brain. Increased pressure in these veins is propagated to the brain and counteracts cerebral arterial blood flow (cerebral blood flow is determined by the gradient [difference] between cerebral arterial and venous pressure). This is one of the major challenges in improving resuscitation outcomes. Various experiments (e.g. head tilting, passive leg raising, etc) have been tried to improve cerebral perfusion during CPR (Debaty et al, Youcef et al).

The compression phase
Chest compressions reduce thoracic volume and increase thoracic pressure. This leads to compression of all structures, including the atria, ventricles, airways, and large vessels. The heart is squeezed between the sternum and the vertebral column, and blood is forced in anterograde direction. Provided that the valvular apparatus is functioning normally, blood is only ejected in anterograde direction, such that the pressure is not transduced to the large veins (which would counteract arterial blood flow).
Coronary perfusion pressure (CPP)
Coronary perfusion is fundamental for restoring and maintaining cardiac electrical activity. Studies demonstrate that a coronary perfusion pressure (CPP) of 15 mmHg is required to induce electrical activity in the myocardium (Paradis et al). The coronary perfusion pressure (CPP) can be calculated as follows:
CPP = Paorta – RAP
Paorta is the intra-aortic pressure (where the coronary arteries originate)
RAP is right atrial pressure (where venous coronary blood is emptied)
However, CPP is approximately 0 mmHg (i.e there is no coronary blood flow) during the compression phase, which is explained by the fact that the pressure is equally elevated in the aorta and the right atrium. Coronary blood flow occurs during the decompression phase (“CPR diastole”). Thoracic volume expands rapidly during the decompression. Right atrial, right ventricular, and left ventricular pressure drops abruptly, but the closing of the aortic valve allows the intra-aortic pressure to remain high. The resulting pressure difference between right atrial pressure (RAP) and intra-aortic pressure (Paorta) is the CPP. The decrease in right atrial pressure and ventricular pressure is also important because it allows for passive flow of blood to the atria and ventricles (Halperin et al).

CPP is very sensitive to interruptions in the compressions. Brief interruptions (seconds) abolish the CPP completely and it takes around 15 compressions to re-establish the CPP after an interruption (Steet et al, Berg et al). This is reflected in animal studies demonstrating that survival decreased by 7% for every 5 seconds of pause before defibrillation (Cheskes et al).
Because coronary perfusion occurs during the decompression phase, effective decompression is essential to generate high CPP and maximize passive reflow to the heart (Niemann et al).
The compressions also lead to increased pressure in the veins in the thorax (paravertebral veins, epidural veins) and the spinal fluid. Unfortunately, this increase in pressure is propagated to the brain and leads to an increase in venous cerebral pressure, and subsequently increased intracranial pressure (ICP). High ICP counteracts the cerebral perfusion pressure (CerPP). Thus, compressions lead to increased intracranial pressure (ICP), which reduces cerebral perfusion (CerPP). Yet, it is essential to generate a high CPP as it is required to induce cardiac activity.
During the compression phase, passive expiration occurs as the lung tissue is compressed. This enables minimal gas exchange. The effectiveness of this gas exchange diminishes gradually unless positive pressure ventilation (PPV) is provided. This is explained by the fact that PPV expands the pulmonary tissue – including bronchioles, arteries and veins – and thus lowers resistance in these compartments.

The decompression phase
During decompression, a passive recoil (expansion) of the thorax occurs. This leads to a rapid decrease in intrathoracic pressure. The resulting vacuum in the lungs draws air into the alveoli. The right and left ventricles are passively filled with blood (mainly because low right-sided pressure causes venous return to the right atrium and ventricle). Decompression also reduces ICP (through the reduction of pressure in the intrathoracic veins draining the head) and thereby facilitates cerebral perfusion during the next compression phase.

Interventions that amplify the recoil (expansion of the thorax) will result in improved preload (ventricular filling) and subsequently larger stroke volumes during the compression phase. CPP will also increase. There is ongoing development of devices that improve recoil through various means. Active decompression through suction devices (e.g. the suction cup on LUCAS) is already in use (Figure 9).

Leaning on the chest during decompression can be fatal. Animal studies show that recoil of 75% (compared to 100%) reduces CPP by approximately 30% and CerPP by 50% (Yannopoulos et al). Observational studies show that leaning occurs in over 90% of cases (Fried et al).
The ventilation phase
Ventilation during CPR is performed with positive pressure ventilation (PVV), forcing air into the lungs. This differs significantly from normal respiration, during which the chest wall is expanded using respiratory muscles. The latter creates a negative intrathoracic pressure, with the resulting vacuum drawing air into the alveoli so that gas exchange can take place. The respiratory muscles are paralyzed during cardiac arrest so PPV is the only possibility to achieve ventilation.
There is evidence that ventilation is less important than compression. Survival is virtually impossible without compressions (CPP must reach 15 mmHg to induce cardiac electrical activity). Ventilation is less critical during the first 4–5 minutes. Several studies have tested compression-only CPR, which entails deferring ventilations during the initial phase. In a large Swedish randomized study, there was no difference in survival when bystanders performed compression-only CPR compared to standard CPR for out-of-hospital cardiac arrest (Svensson et al). Similar results were reported in a large observational study (Jerkeman et al). As mentioned above, compressions result in some, albeit minimal, ventilation (McDannold et al). Yet, positive pressure ventilation is recommended as soon as possible because the effectiveness of the compressions diminishes after a few minutes of compressions. This is explained by the fact that the pulmonary vessels and bronchioles collapse gradually during the compression phase (Dunnham-Snary et al). To expand the pulmonary vessels and bronchioles, positive pressure ventilation must be performed (Markstaller et al).
Hyperventilation must always be avoided during cardiopulmonary resuscitation. It prevents the pressure drop in the thorax, which counteracts the passive filling. Hyperventilation also leads to increased right atrial pressure during diastole, which reduces CPP. In an animal study, CPP decreased by 28% during hyperventilation (Aufderheide et al). Hyperventilation is also unnecessary because cardiac output is low during CPR, which means that small tidal volumes are sufficient to eliminate CO2 and oxygenate the blood.

References
Keith G. Lurie, MD, Edward C. Nemergut, MD, Demetris Yannopoulos, MD, and Michael Sweeney, MD. The Physiology of Cardiopulmonary Resuscitation. Anesthesia and analgesia (2015).
Duggal C, Weil MH, Gazmuri RJ, Tang W, Sun S, O’Connell F, Ali M. Regional blood flow during closed-chest cardiac resuscitation in rats. J Appl Physiol 1993;74:147–52.
Matilda Jerkeman, Peter Lundgren, Elmir Omerovic, Anneli Strömsöe, Gabriel Riva, Jacob Hollenberg, Per Nivedahl, Johan Herlitz, Araz Rawshani. Association between type of bystander cardiopulmonary resuscitation and survival in out-of-hospital cardiac arrest: A machine learning studyResuscitation Plus. 2022 Jun 14;10:100245.
Debaty G, Shin SD, Metzger A, Kim T, Ryu HH, Rees J, McKnite S, Matsuura T, Lick M, Yannopoulos D, Lurie K. Tilting for perfusion: head-up position during cardiopulmonary resuscitation improves brain flow in a porcine model of cardiac arrest. Resuscitation 2015;87:38–43.
Stiell IG, Brown SP, Christenson J, Cheskes S, Nichol G, Powell J, Bigham B, Morrison LJ, Larsen J, Hess E, Vaillancourt C, Davis DP, Callaway CW; Resuscitation Outcomes Consortium (ROC) Investigators. What is the role of chest compression depth during out-of-hospital cardiac arrest resuscitation? Crit Care Med 2012;40:1192–8 8.
Idris AH, Guffey D, Aufderheide TP, Brown S, Morrison LJ, Nichols P, Powell J, Daya M, Bigham BL, Atkins DL, Berg R, Davis D, Stiell I, Sopko G, Nichol G; Resuscitation Outcomes Consortium (ROC) Investigators. Relationship between chest compression rates and outcomes from cardiac arrest. Circulation 2012;125:3004–12
Sue Duval, Paul E. Pepe, MD, MPH2,3,4,5,6; Tom P. Aufderheide, MD, MS7; et alJeffrey M. Goodloe, MD8; Guillaume Debaty, MD, PhD9,10; José Labarère, MD, PhD9,10; Atsushi Sugiyama, MD, PhD11; Demetris Yannopoulos, MD1 Optimal Combination of Compression Rate and Depth During Cardiopulmonary Resuscitation for Functionally Favorable Survival. JAMA Cardiol. 2019;4(9):900-908. doi:10.1001/jamacardio.2019.2717
Bobrow BJ, Spaite DW, Berg RA, et al. Chest compression-only CPR by lay rescuers and survival from out-of-hospital cardiac arrest. JAMA. 2010;304(13):1447-1454.
Markstaller K, Rudolph A, Karmrodt J, et al. Effect of chest compressions only during experimental basic life support on alveolar collapse and recruitment. Resuscitation. 2008;79(1):125-132.
McDannold R, Bobrow BJ, Chikani V, Silver A, Spaite DW, Vadeboncoeur T. Quantification of ventilation volumes produced by compressions during emergency department cardiopulmonary resuscitation. Am J Emerg Med. 2018;36(9):1640-1644.
Dunham-Snary KJ, Wu D, Sykes EA, et al. Hypoxic Pulmonary Vasoconstriction: From Molecular Mechanisms to Medicine. Chest. 2017;151(1):181-192.
List of authors. Leif Svensson, M.D., Ph.D., Katarina Bohm, R.N., Ph.D., Maaret Castrèn, M.D., Ph.D., Hans Pettersson, Ph.D., Lars Engerström, M.D., Johan Herlitz, M.D., Ph.D., and Mårten Rosenqvist, M.D., Ph.D. Compression-Only CPR or Standard CPR in Out-of-Hospital Cardiac Arrest. New England Journal of Medicine (2018).
Youcef Azeli, Alfredo Bardají, Eneko Barbería, Vanesa Lopez-Madrid, Jordi Bladé-Creixenti, Laura Fernández-Sender, Gil Bone, Elena Rica Susana Álvarez 11, Alberto Fernández, Christer Axelsson, Maria F Jiménez-Herrera. Clinical outcomes and safety of passive leg raising in out-of-hospital cardiac arrest: a randomized controlled trial. Critical Care (2021).
Duggal C, Weil MH, Gazmuri RJ, Tang W, Sun S, O’Connell F, Ali M. Regional blood flow during closed-chest cardiac resuscitation in rats. J Appl Physiol 1993;74:147–52
Aufderheide TP, Sigurdsson G, Pirrallo RG, et al. Hyperventilation-induced hypotension during cardiopulmonary resuscitation. Circulation 2004;109:1960–5.
Debaty G, Shin SD, Metzger A, Kim T, Ryu HH, Rees J, McKnite S, Matsuura T, Lick M, Yannopoulos D, Lurie K. Tilting for perfusion: head-up position during cardiopulmonary resuscitation improves brain flow in a porcine model of cardiac arrest. Resuscitation 2015;87:38–43
Niemann JT. Differences in cerebral and myocardial perfusion during closed-chest resuscitation. Ann Emerg Med 1984;13:849–53
Halperin HR, Tsitlik JE, Guerci AD, et al. Determinants of blood flow to vital organs during cardiopulmonary resuscitation in dogs. Circulation 1986;73:539–50.
Paradis NA, Martin GB, Rivers EP, et al. Coronary perfusion pressure and the return of spontaneous circulation in human cardiopulmonary resuscitation. JAMA 1990;263:1106–13.
Stiell IG, Brown SP, Christenson J, Cheskes S, Nichol G, Powell J, Bigham B, Morrison LJ, Larsen J, Hess E, Vaillancourt C, Davis DP, Callaway CW; Resuscitation Outcomes Consortium (ROC) Investigators. What is the role of chest compression depth during out-of-hospital cardiac arrest resuscitation? Crit Care Med 2012;40:1192–8 8.
Idris AH, Guffey D, Aufderheide TP, Brown S, Morrison LJ, Nichols P, Powell J, Daya M, Bigham BL, Atkins DL, Berg R, Davis D, Stiell I, Sopko G, Nichol G; Resuscitation Outcomes Consortium (ROC) Investigators. Relationship between chest compression rates and outcomes from cardiac arrest. Circulation 2012;125:3004–12
Cheskes S, Schmicker RH, Verbeek PR, et al. ThE impact of peri-shock pause on survival from out-of-hospital shockable cardiac arrest during the resuscitation outcomes consortium PRIMED trial. Resuscitation 2014;85:336–42.
Bobrow BJ, Spaite DW, Berg RA, et al. Chest compression-only CPR by lay rescuers and survival from out-of-hospital cardiac arrest. JAMA – J Am Med Assoc. 2010;304(13):1447-1454.
Markstaller K, Rudolph A, Karmrodt J, et al. Effect of chest compressions only during experimental basic life support on alveolar collapse and recruitment. Resuscitation. 2008;79(1):125-132.
McDannold R, Bobrow BJ, Chikani V, Silver A, Spaite DW, Vadeboncoeur T. Quantification of ventilation volumes produced by compressions during emergency department cardiopulmonary resuscitation. Am J Emerg Med. 2018;36(9):1640-1644.
Dunham-Snary KJ, Wu D, Sykes EA, et al. Hypoxic Pulmonary Vasoconstriction: From Molecular Mechanisms to Medicine. Chest. 2017;151(1):181-192.
Compression-Only CPR or Standard CPR in Out-of-Hospital Cardiac Arrest List of authors. Leif Svensson, M.D., Ph.D., Katarina Bohm, R.N., Ph.D., Maaret Castrèn, M.D., Ph.D., Hans Pettersson, Ph.D., Lars Engerström, M.D., Johan Herlitz, M.D., Ph.D., and Mårten Rosenqvist, M.D., Ph.D
Steen S, Liao Q, Pierre L, et al. The critical importance of minimal delay between chest compressions and subsequent defibrillation: a haemodynamic explanation. Resuscitation 2003;58:249–58. 19
Berg RA, Sanders AB, Kern KB, et al. Adverse hemodynamic effects of interrupting chest compressions for rescue breathing during cardiopulmonary resuscitation for ventricular fibrillation cardiac arrest. Circulation 2001;104:2465–70.
Yannopoulos D, McKnite S, Aufderheide TP, et al. Effects of incomplete chest wall decompression during cardiopulmonary resuscitation on coronary and cerebral perfusion pressures in a porcine model of cardiac arrest. Resuscitation 2005;64:363–72.
Fried DA, Leary M, Smith DA, et al. The prevalence of chest compression leaning during in-hospital cardiopulmonary resuscitation. Resuscitation 2011;82:1019–24.

