Capnography (end-tidal carbon dioxide measurement, ETCO2) during cardiac arrest
Capnography (end-tidal carbon dioxide, ETCO2)
Capnography refers to the measurement of end-tidal carbon dioxide (ETCO2) in the respiratory system. ETCO2 is the partial pressure of carbon dioxide (CO2) at the end of expiration. It provides an integrated view of ventilation, metabolism, and perfusion. Carbon dioxide, a byproduct of aerobic metabolism, is transported from the tissues back to the lungs where it is exhaled. The final partial pressure of carbon dioxide in exhaled air represents the sum of ventilation, metabolic activity, and perfusion. Increased aerobic metabolism, perfusion, and ventilation result in a higher end-tidal carbon dioxide level. Continuous ETCO2 monitoring is possible by means of intubation and ventilation devices equipped with sensors. A normal capnogram is depicted in Figure 1.
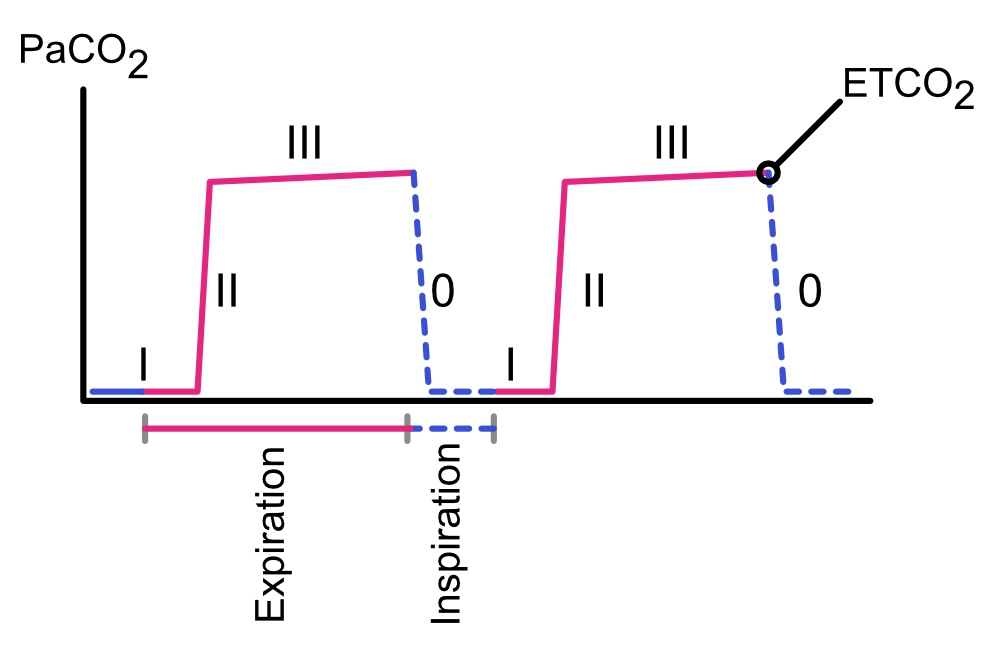
- Phase I (Inspiratory Baseline): Reflects inhaled air devoid of CO2.
- Phase II (Rapid Expiration): Represents the transition of air from anatomical dead space to functional alveolar space.
- Phase III (Alveolar Plateau): ETCO2 is the recorded CO2 partial pressure just before the next inspiration.
- Phase 0: Indicates the beginning of the next inspiration.
Normal ETCO2: 38 mmHg (5 kPa) or 5%.
Monitoring ETCO2 aids in:
- Assessing ventilation quality.
- Determining ventilation rate.
- Verifying the position of the tracheal tube.
- Evaluating the efficacy of chest compressions.
- Identifying return of spontaneous circulation (ROSC).
- Prognostication.
Potential reasons for a flat ETCO2 curve include:
- Ventilator or capnograph not activated.
- Displacement of the tracheal tube.
- Cardiac arrest without adequate blood flow or ineffective compressions.
While ETCO2 is optimally measured in tracheal tubes, it can also be gauged through supraglottic airway devices and Rubens’ tubes. Following ROSC, ETCO2 can rise up to threefold from levels observed during compressions. A sudden increase in ETCO2 indicates either ROSC or an adjusted tube placement. Often, a rise in ETCO2 is observed before a detectable pulse post-ROSC.
If ETCO2 remains below 1.33 kPa (10 mmHg) during CPR, it indicates a dismal prognosis. This threshold may trigger consideration for Extracorporeal Membrane Oxygenation (ECMO) initiation (Soar et al). ETCO2 trends can vary during CPR depending on various factors such as the cause of cardiac arrest, compression efficacy, ventilation depth and frequency, and adrenaline administration. Therefore, it is advised to use ETCO2 trends over time rather than single measurements. ETCO2 should not be the sole determinant for terminating CPR or initiating ECMO (Paiva et al).
If both ETCO2 and other indicators suggest ROSC, compressions may be temporarily paused.

