Physiological Assessment of Coronary Stenoses and Revascularization Decisions
Abstract
Angiographic stenosis severity is a poor surrogate for the hemodynamic significance of a coronary lesion, with anatomic and functional assessment discordant in a substantial minority of intermediate lesions. Over the past three decades, invasive physiological indices, led by fractional flow reserve (FFR), have been validated against outcomes and shown to outperform visual angiographic guidance in selecting lesions for percutaneous coronary intervention (PCI). Non hyperemic pressure ratios (instantaneous wave free ratio [iFR], resting full cycle ratio [RFR], and related resting indices) simplified the procedure by removing the need for pharmacologic hyperemia, and angiography derived indices (quantitative flow ratio [QFR], FFRangio, and three dimensional quantitative coronary angiography based vessel FFR) have more recently removed the need for a pressure wire altogether. In parallel, large outcome trials have clarified, and in some cases substantially narrowed, the role of revascularization itself in stable coronary artery disease, while a distinct evidence base has emerged for coronary microvascular and vasospastic disease using coronary flow reserve (CFR) and the index of microcirculatory resistance (IMR). This review synthesizes the physiological basis, diagnostic performance, and outcome evidence for each index, situates two recent noninferiority trials of wire free angiography derived physiology (ALL-RISE and FAST III) within this evolving landscape, and proposes an integrated decision pathway for physiology guided revascularization.
Overview: Comparison of Physiological Indices
The table below summarizes the four index families discussed in this review, mechanism, principal advantages, principal limitations, and the key trials supporting each. A more detailed mechanistic discussion of each index follows in Section 2, and a guideline oriented comparison (procedural requirements, validated cutoffs, current guideline recommendation class) appears in Section 6.
| Index | Mechanism | Advantages | Limitations | Key evidence |
|---|---|---|---|---|
| Fractional Flow Reserve (FFR) | Ratio of distal coronary pressure (Pd) to aortic pressure (Pa) at maximal pharmacologic hyperemia (adenosine); approximates fraction of normal maximal flow preserved by the stenosis. Cutoff ≤ 0.80. | Deepest outcome-trial evidence base of any physiological index; lesion-specific and largely independent of resting hemodynamics; guideline reference standard. | Requires pressure wire + vasodilator (cost, time, patient discomfort); falsely normal in microvascular dysfunction (diabetes, LVH, aortic stenosis, post-MI stunning); blind to microvascular disease by design; low real-world adoption. | DEFER (15-yr) · FAME · FAME 2 (5-yr, 11-yr) · FAME 3 |
| Non-hyperemic ratios (iFR / RFR / Pd-Pa / dPR) | Resting Pd/Pa during the diastolic “wave-free period” (iFR) or the lowest ratio across the full cardiac cycle (RFR); no vasodilator. Cutoff ≤ 0.89. | No hyperemic agent — faster, cheaper, better tolerated; validated in large 1-year outcome trials as noninferior to FFR; enables hybrid gray-zone strategies (measure FFR only when iFR/RFR is indeterminate). | Resting resistance only approximates hyperemic resistance — ~15–20% discordance with FFR classification; pooled 5-year follow-up showed higher all-cause mortality vs FFR-guided care despite 1-year noninferiority. | DEFINE-FLAIR · iFR-SWEDEHEART · 5-yr pooled analysis · VALIDATE-RFR |
| Coronary Flow Reserve (CFR) & Index of Microcirculatory Resistance (IMR) | CFR: ratio of hyperemic to resting coronary flow/velocity (Doppler or thermodilution wire) — reflects combined epicardial + microvascular resistance. IMR: distal pressure × hyperemic mean transit time — isolates microvascular resistance. | Only indices that detect microvascular disease as an independent cause of ischemia, including with non-obstructive epicardial arteries (ANOCA/INOCA); CFR has independent prognostic value. | CFR confounded by heart rate/blood pressure/contractility (less reproducible, less lesion-specific); no sharp normal cutoff; technically demanding acquisition; CFR alone cannot localize epicardial vs microvascular cause without paired FFR/IMR. | CorMicA (stratified medicine trial) |
| Angiography-derived / wire-free (QFR, FFRangio, vessel-FFR) | 3-D reconstruction of the vessel from ≥25°-separated angiographic projections; FFR-equivalent computed via frame-counting flow estimation (QFR) or computational fluid dynamics with modeled/measured hyperemic pressure. No pressure wire; most platforms need no vasodilator. Cutoff ≤ 0.80. | Removes wire-related risk (spasm, dissection, drift) and most/all hyperemic-agent burden; can be computed retrospectively from existing angiograms, lowering marginal cost of assessment; QFR now noninferior/superior to angiography-guided care in large outcome trials; FFRangio and vessel-FFR now shown noninferior to pressure-wire FFR itself. | Accuracy depends on angiographic image quality — studies exclude high-single- to high-teens-% of vessels for suboptimal imaging; degraded performance in ostial lesions, tortuosity, diffuse or serial disease, and near the 0.80 cutoff; higher test-retest variability than repeated pressure-wire FFR; accuracy of one platform does not transfer to another (each requires its own outcome trial). | FAVOR III China (QFR, 2-yr) · ALL-RISE (FFRangio vs wire-FFR) · FAST III (vessel-FFR vs wire-FFR) |
Introduction: why physiology, not just anatomy
Coronary angiography depicts lumen silhouette, not the hemodynamic consequence of a stenosis. Diffuse disease, eccentric plaque, foreshortening, and vessel overlap all degrade the correlation between percent diameter stenosis and the pressure or flow drop it produces, and angiographic and functional severity are discordant in a large proportion of intermediate lesions [3]. FFR guided PCI has repeatedly shown better clinical outcomes than standard angiography guided PCI, establishing that functional rather than anatomic significance should define the revascularization decision [3,4].
This discordance matters clinically because unnecessary stenting of non ischemic lesions exposes patients to procedural risk, stent thrombosis, and restenosis without a corresponding reduction in events, while deferring a truly flow limiting lesion leaves the patient under treated. The physiological indices reviewed here were each developed to close the gap between what the angiogram shows and what the lesion actually does to myocardial blood supply.
The core physiological indices
Each index below answers a related but distinct physiological question, is the epicardial stenosis flow limiting under near maximal demand, is it flow limiting at rest, is the whole coronary bed (epicardial plus microvascular) able to augment flow, or is the microcirculation itself dysfunctional. None is a drop in replacement for the others; they trade off invasiveness, procedural burden, and what physiological question they actually answer. Table 1 (Section 6) summarizes these trade offs; this section explains the mechanistic basis for each.
Fractional flow reserve (FFR)
Mechanism. FFR is the ratio of mean distal coronary pressure (Pd) to mean aortic pressure (Pa) measured across a stenosis during maximal, pharmacologically induced hyperemia (typically intravenous or intracoronary adenosine). Flow through a coronary bed is approximated as the pressure difference across it divided by the resistance of the microvasculature; the entire logic of FFR rests on the assumption that during maximal hyperemia, microvascular resistance is minimized and behaves the same as it would in an equivalent, disease free artery, so that resistance cancels out of the ratio and the pressure ratio alone stands in for the flow ratio [25,29]. Under this assumption, FFR approximates the fraction of normal maximal myocardial blood flow that is still achievable in the presence of the stenosis: an FFR of 0.70 means the vessel can deliver only 70% of the flow it would without the lesion. A cutoff of ≤0.80 defines hemodynamic significance, with a recognized gray zone between 0.75 and 0.80 [1,2].
Advantages. FFR is lesion specific, because the calculation is normalized to the same vessel’s own hypothetical disease free flow, it isolates the epicardial stenosis from the rest of the coronary tree, is largely independent of resting hemodynamics (heart rate, blood pressure, contractility), and is highly reproducible [25]. It is the index with the deepest outcome evidence base of any physiological measurement in cardiology (Section 3), and current guidelines therefore treat it as the reference standard against which every newer index is validated.
Limitations. The entire calculation is built on an assumption that can fail: in patients with substantial coronary microvascular dysfunction, seen with diabetes, longstanding hypertension, left ventricular hypertrophy, aortic stenosis, or microvascular stunning after myocardial infarction, the hyperemic response is blunted, this violates the “minimal and constant microvascular resistance” assumption, and can produce a falsely normal (elevated) FFR that under calls a genuinely flow limiting stenosis [25,26,29]. Achieving true maximal hyperemia also depends on adequate adenosine dosing and delivery; submaximal hyperemia biases FFR upward for the same underlying reason. FFR requires a pressure wire, intracoronary or intercoronary vasodilator administration, and the associated cost, procedural time, and patient discomfort (flushing, dyspnea, transient AV block) that come with pharmacologic hyperemia, the practical burden most directly responsible for its persistently low real world adoption despite three decades of outcome evidence [23]. Because FFR is calculated assuming negligible central venous pressure, states of elevated right atrial pressure (e.g., severe pulmonary hypertension, right heart failure) can introduce a small but occasionally consequential error very close to the 0.80 cutoff [26]. Finally, FFR characterizes the epicardial lesion in isolation from the microcirculation by design, it cannot detect microvascular disease as a cause of ischemia in a vessel with no obstructive epicardial stenosis, which is precisely the gap that CFR/IMR testing is designed to fill (Section 2.3).
Non hyperemic pressure ratios (iFR, RFR, Pd/Pa, dPR)
Mechanism. The instantaneous wave free ratio (iFR) measures the resting Pd/Pa ratio during a specific window in diastole, the “wave free period”, during which no new pressure wavefronts are generated by ventricular contraction and coronary autoregulation has already reduced microvascular resistance to a level that approximates (though does not exactly replicate) the resistance achieved during pharmacologic hyperemia [11,27]. In effect, the wave free period substitutes a naturally occurring low and stable resistance interval for the pharmacologically induced one that FFR requires, permitting an FFR like pressure ratio to be extracted without adenosine [27]. The resting full cycle ratio (RFR) generalizes this idea by scanning the entire cardiac cycle, not only the diastolic wave free window, for the single lowest Pd/Pa value, on the premise that this minimum will fall within or close to the wave free period in the great majority of physiological states and can therefore serve the same diagnostic purpose without being tied to a fixed anatomical window of diastole. Resting (whole cycle) Pd/Pa and the diastolic pressure ratio (dPR) are close technical relatives that average or restrict the same resting pressure signal differently.
Advantages. None of these indices requires pharmacologic hyperemia, which removes adenosine related cost, procedural time, and patient discomfort, and removes any risk associated with the vasodilator itself (flushing, transient dyspnea, bronchospasm in reactive airway patients, and rare AV block) [11]. This has made them attractive as a default first assessment, with FFR reserved for equivocal cases in “hybrid” decision strategies (e.g., defer if iFR >0.93, treat if <0.86, measure FFR only in the 0.86 to 0.93 gray zone) [28]. DEFINE-FLAIR and iFR-SWEDEHEART established 1 year clinical noninferiority of iFR against FFR at large scale (Section 3.4), and VALIDATE-RFR established near equivalence of RFR to iFR [13].
Limitations. Because the wave free period is a physiological, not fixed anatomical, interval, its resistance is only an approximation of true hyperemic resistance, not an identical state, the two indices are measuring genuinely different physiological conditions (resting autoregulated flow vs. pharmacologically maximized flow), and this is the root cause of a well documented discordance between iFR and FFR classification in roughly 15 to 20% of lesions, not measurement noise alone [12,29]. This discordance is clinically consequential in the minority of cases where iFR calls a lesion non significant, but FFR would call it significant (or vice versa), because it can lead to a different revascularization decision depending purely on which index was used. The longer term, pooled 5 year follow up of DEFINE-FLAIR and iFR-SWEDEHEART reported higher all cause mortality with iFR guided care compared with FFR guided care despite 1 year noninferiority (Section 3.4), a signal that has renewed scrutiny of whether resting state assessment fully substitutes for a hyperemic one in every patient [12]. Non hyperemic indices also inherit standard pressure wire risks (wire induced spasm or dissection, drift) and, like FFR, assume negligible central venous pressure.
Coronary flow reserve (CFR) and index of microcirculatory resistance (IMR)
Mechanism. CFR is the ratio of coronary blood flow (or flow velocity) at maximal hyperemia to flow at rest, measured with a Doppler tipped or thermodilution capable pressure wire. Unlike FFR, which is normalized against a hypothetical disease free version of the same vessel, CFR is a direct, unnormalized measurement of how much a given vessel’s flow can be augmented, a quantity that reflects the combined resistance of the epicardial stenosis and the microcirculation downstream of it, without distinguishing between the two [29]. IMR isolates the microvascular component: using the same thermodilution capable wire, IMR is calculated from the distal coronary pressure and the mean transit time of a saline bolus at maximal hyperemia, producing an estimate of minimal microvascular resistance that is far less confounded by the epicardial stenosis than CFR is.
Advantages. Because CFR and IMR characterize the coronary circulation as a whole (CFR) or the microcirculation specifically (IMR), they are the only indices in this review capable of detecting microvascular disease as an independent cause of angina or ischemia, including in vessels with no obstructive epicardial stenosis at all, precisely the ANOCA/INOCA population that FFR, iFR, RFR, and angiography derived indices cannot characterize by design, since all of those are constructed specifically to isolate the epicardial lesion from the microcirculation [19,29]. CFR has separate, validated prognostic value: a depressed CFR predicts adverse cardiac events even when the epicardial stenosis itself is not flow limiting [29].
Limitations. CFR is a ratio of resting to hyperemic flow, so it is directly sensitive to whatever resting flow happens to be at the time of measurement, heart rate, blood pressure, and left ventricular contractility all shift the denominator and can move CFR substantially without any change in the underlying stenosis or microvasculature, which is why CFR is considered less reproducible and less lesion specific than FFR [29]. There is no single, universally agreed normal cutoff (values below 2.0 are commonly treated as abnormal, but the transition is not sharp), which complicates its use for a binary treat/defer decision in isolation [29]. Doppler based CFR measurement is technically demanding, obtaining a stable, high quality flow velocity signal requires operator experience, and signal dropout is common, while thermodilution based CFR and IMR require specific compatible pressure wires and add procedural time and cost beyond a standard FFR pullback. Finally, because CFR conflates epicardial and microvascular resistance, an abnormal CFR alone cannot say which compartment is responsible without a paired FFR (or IMR) measurement in the same vessel, the rationale for measuring FFR, CFR, and IMR together, as in the CorMicA protocol (Section 5), rather than any single one in isolation [19].
Angiography derived / wire free physiology (QFR, FFRangio, vessel FFR)
Mechanism. This newest class of indices reconstructs the coronary artery in three dimensions from two (or more) standard angiographic projections acquired at least ~25° apart, then computes an FFR equivalent pressure ratio along that reconstructed lumen using computational flow modeling, without a physical pressure wire in the vessel. Platforms differ in how they estimate flow: quantitative flow ratio (QFR) infers flow velocity from the rate of contrast movement through the vessel on the existing angiographic runs (frame counting), while some other angiography derived and vessel FFR platforms couple the 3D reconstruction with computational fluid dynamics and either a modeled or a measured (aortic catheter) hyperemic pressure, without requiring the vasodilator drug itself in most implementations [20].
Advantages. Removing the pressure wire removes the small but real risks of wire induced coronary spasm, dissection, and drift, along with the added contrast, fluoroscopy, and procedural time of a wire pullback; removing the need for adenosine (where applicable) removes the drug related discomfort and cost as well. Because these indices can, in principle, be computed retrospectively from angiograms already acquired for diagnostic purposes, they lower the marginal cost of obtaining a physiological assessment to near zero for any patient with adequate quality angiographic images, directly addressing the low real world uptake of pressure wire physiology noted throughout this review [23]. QFR in particular now has a large outcome evidence base (FAVOR III China and its 2 year follow up; Section 3.5), and ALL-RISE and FAST III extend this class of evidence to FFRangio and 3D QCA based vessel FFR, respectively, each showing 1 year noninferiority against pressure wire FFR itself [23,24].
Limitations. Diagnostic accuracy is contingent on angiographic image quality in a way that pressure wire measurement is not: suboptimal lesion visualization, inadequate contrast filling, vessel overlap or foreshortening, and insufficient separation between the two acquisition angles all degrade the 3D reconstruction and the resulting flow computation, and validation studies routinely exclude a meaningful fraction of vessels (commonly reported in the high single digits to high teens of percent) for exactly these reasons [20,21,26]. Diagnostic performance is measurably lower in technically difficult anatomy, ostial lesions, severely tortuous vessels, diffuse disease, and tandem/serial lesions, and in the “gray zone” near the 0.80 cutoff itself, where small errors in the reconstruction are most likely to change the treat/defer classification [20,22,27]. Reported test retest variability for QFR is larger than that of repeated pressure wire FFR, meaning two analyses of the same angiographic run can disagree by more than repeated wire based measurements would [21]. Because platforms differ in whether they measure or model hyperemic flow, accuracy claims from one angiography derived platform (e.g., QFR) do not automatically transfer to another (e.g., FFRangio or a different vessel FFR implementation), each requires its own outcome evidence, which is exactly why ALL-RISE and FAST III were necessary trials rather than redundant confirmations of FAVOR III China.
Landmark outcome evidence linking physiology to revascularization
DEFER: the foundational deferral trial
The DEFER trial, first reported in 2001, established that lesions with a normal FFR could be safely left unstented [1]. It was the first randomized trial to demonstrate that deferring PCI for intermediate stenoses with FFR >0.75 was safe; at 15 year follow up, event rates remained low in the deferred group with no excess in death or myocardial infarction compared with the revascularized group, providing the earliest evidence against a late “catch up” phenomenon [2]. In the formal 15 year report, complete follow up was obtained in 92% of patients, and the rate of death was not different between the deferred group (33.0%) and the revascularized group (31.1%; relative risk 1.06, 95% CI 0.69 to 1.62, P=0.79) [2].
FAME and FAME 2: FFR guided PCI versus angiography and versus medical therapy
FAME (2009) randomized 1005 patients with multivessel disease to angiography guided or FFR guided PCI (stenting only if FFR ≤0.80); the 1 year primary end point of death, MI, or repeat revascularization occurred in significantly fewer patients in the FFR guided arm (13.2% vs 18.3%, P=0.02) [3], with benefit sustained through 2 year and 5 year follow up [4,5].
FAME 2 (2012) asked a different question: among patients with at least one hemodynamically significant stenosis, does FFR guided PCI added to medical therapy outperform medical therapy alone? PCI performed to contemporary quality standards plus best available medical therapy resulted in significantly improved clinical outcomes compared with medical therapy alone, driven by an eight fold increase in the need for urgent revascularization in the medical therapy group [6]. The trial was in fact stopped early after its independent data and safety monitoring board found a significant reduction in unplanned hospital readmission and urgent revascularization with FFR guided PCI, deeming it unjustifiable to continue randomizing patients to medical therapy alone [6]. At 5 year follow up, FFR guided PCI led to a significantly lower rate of the composite primary end point (death, myocardial infarction, or urgent revascularization) than medical therapy alone [7], and the most recent 11 year follow up (Nature Medicine, 2026) reported a win ratio of 1.25 in favor of PCI (95% CI 1.01 to 1.56, P=0.043; number needed to treat 17), driven primarily by a large reduction in urgent revascularizations (win ratio 4.57, 95% CI 2.53 to 8.24) [8].
FAME 3: FFR guided PCI versus CABG
FAME 3 (2022) tested whether contemporary FFR guided PCI, using current generation drug eluting stents, could match surgical revascularization in three vessel disease, a comparison earlier trials had not made with FFR guided lesion selection [9]. The trial informs, rather than eliminates, the anatomic decision between PCI and CABG in complex multivessel disease.
Non hyperemic indices: DEFINE-FLAIR and iFR-SWEDEHEART
Two large trials in 2017 tested whether iFR, without hyperemia, could replace FFR for revascularization decisions. In DEFINE-FLAIR, 2492 patients were randomly assigned 1:1 to iFR guided or FFR guided revascularization, with a prespecified noninferiority margin of 3.4 percentage points on the 1 year composite of death, nonfatal MI, or unplanned revascularization; the primary end point occurred in 6.8% of the iFR group versus 7.0% of the FFR group, meeting noninferiority, with fewer adverse procedural signs/symptoms and a shorter procedure with iFR [10]. iFR-SWEDEHEART reported concordant 1 year noninferiority in an independent cohort [11].
Longer follow up introduced a note of caution, however. A pooled 5 year analysis of both trials found that iFR guided revascularization was associated with an increase in the composite of MACE (all cause mortality, MI, or unplanned revascularization) and in all cause mortality alone compared with FFR guided revascularization, while rates of MI and unplanned revascularization alone did not differ [12]. This mortality signal has not been definitively explained and has not (yet) changed guideline level equivalence between the two indices, but it is a live point of debate that any physiology guided pathway should acknowledge rather than gloss over.
Angiography derived / wire free physiology: FAVOR III China, ALL-RISE, and FAST III
FAVOR III China provided the first large outcome trial of an angiography derived index, QFR. Among 3825 patients undergoing PCI, a QFR guided strategy of lesion selection improved 1 year clinical outcomes compared with standard angiography guidance: the primary end point occurred in 5.8% of the QFR guided group versus 8.8% of the angiography guided group (hazard ratio 0.65, 95% CI 0.51 to 0.83, P=0.0004), driven by fewer myocardial infarctions and ischemia driven revascularizations [20]. This benefit was durable, with 2 year MACE of 8.5% versus 12.5% (hazard ratio 0.66, 95% CI 0.54 to 0.81, P<0.0001) [21].
Two further noninferiority trials, specified for inclusion in this review, extend wire free physiology to platforms that test angiography derived FFR head to head against the pressure wire standard, rather than against angiography alone.
ALL-RISE compared FFRangio, an angiography derived index, against conventional pressure wire FFR [23]. A total of 1930 patients undergoing coronary angiography with at least one intermediate stenosis were randomly assigned to physiological assessment with FFRangio (965 patients) or a pressure wire based approach (965 patients). At 1 year, the primary end point (death, myocardial infarction, or unplanned, clinically indicated coronary revascularization) occurred in 6.9% of the FFRangio group and 7.1% of the pressure wire group (hazard ratio 0.98, 95% CI 0.70 to 1.39; P<0.001 for noninferiority against a 3.5 percentage point margin), with no apparent differences in bleeding, acute kidney injury, or procedure related adverse events between groups (ClinicalTrials.gov NCT05893498) [23].
FAST III tested a related but distinct angiography derived approach, vessel FFR (vFFR) derived from three dimensional quantitative coronary angiography without a pressure wire or hyperemic agent, against pressure wire FFR in patients with chronic or acute coronary syndromes and intermediate lesions (30 to 80% diameter stenosis) [24]. The primary end point (death from any cause, any myocardial infarction, or any revascularization at 1 year) was assessed in 1116 patients assigned to vFFR guided revascularization and 1095 assigned to FFR guided revascularization; the event occurred in 7.5% of each group (risk difference −0.02 percentage points, 95% CI −2.25 to 2.21; P=0.004 for noninferiority against a 3.0 percentage point margin), with a similar incidence of serious adverse events (ClinicalTrials.gov NCT04931771) [24].
Taken together, these two trials indicate that angiography derived, wire free physiological assessment, whether FFRangio or 3D QCA based vessel FFR, can match pressure wire FFR for hard clinical outcomes at 1 year, extending the earlier superiority signal from FAVOR III China (QFR vs. angiography alone) to a direct comparison against the invasive reference standard itself. This is a meaningfully higher evidentiary bar than earlier angiography derived validation studies cleared, and it addresses the adoption barrier noted above: a wire free strategy noninferior to pressure wire FFR could substantially widen access to physiological lesion assessment without the cost, time, and hyperemic agent burden of the invasive procedure.
Guideline level integration
The 2024 ESC guidelines for chronic coronary syndromes formalize much of this evidence [22]. Invasive pressure wire assessment of intermediate, non left main stenoses is recommended (Class I, Level A) before a revascularization decision, with FFR (≤0.80) and iFR (≤0.89) as the standard techniques (Class I, Level A). Resting Pd/Pa, dPR, RFR, and angiography derived vessel FFR may be considered as alternative parameters, while systematic, routine wire based assessment of every coronary vessel is not recommended. Among angiography derived options, QFR carries a Class IB recommendation for assessing epicardial stenosis severity and a Class IA recommendation for guiding lesion selection in multivessel disease, whereas other angiography based vessel FFR methods (including FFRangio type and vFFR type platforms) carry a Class IIb/C recommendation, reflecting the smaller accumulated outcome evidence base for those platforms at the time of guideline writing. The ALL-RISE and FAST III results reviewed above are precisely the kind of evidence expected to strengthen the recommendation for those platforms in a future guideline cycle.
Revascularization versus medical therapy: the broader context
Physiological lesion assessment answers which lesions are flow limiting; a separate body of evidence addresses whether revascularizing flow limiting lesions actually improves hard outcomes or symptoms beyond optimal medical therapy, and under what circumstances.
COURAGE (2007) was an early, non physiology guided test of this question, randomizing 2287 patients with stable CAD (selected by angiographic and clinical criteria, not systematic FFR) to PCI plus optimal medical therapy or medical therapy alone. Over a mean follow up of 4.6 years, there was no significant difference between groups in the primary end point of death or myocardial infarction (19% vs 18.5%, P=0.62) [18]. This result helped motivate FAME 2’s hypothesis that selecting patients by FFR documented ischemia, rather than by angiographic severity alone, might reveal a PCI benefit that COURAGE’s unselected population had masked [6].
ISCHEMIA (2020) revisited this question in a larger, more contemporary population with moderate to severe ischemia on stress testing (not invasive FFR), randomizing over 5000 patients to a routine invasive strategy or a conservative, medical therapy first strategy. The trial did not find evidence that an initial invasive strategy reduced the risk of ischemic cardiovascular events or death from any cause compared with a conservative strategy, and the findings were sensitive to the definition of myocardial infarction used [16]. ISCHEMIA did, however, show a health status (angina and quality of life) benefit for the invasive strategy in symptomatic patients: participants in the invasive strategy group had larger improvements in angina related health status than those managed conservatively, with minimal benefit in asymptomatic patients and larger benefit in those with more frequent baseline angina [17].
ORBITA and ORBITA-2 isolated the symptomatic effect of PCI itself using a placebo controlled, blinded design, a methodological step beyond even ISCHEMIA. The original ORBITA, in which guideline directed antianginal medications were mandated in both arms, found no significant effect of PCI on treadmill exercise time versus a placebo (sham) procedure [14], a genuinely surprising result given that enrolled lesions were, by physiological standards, often severely flow limiting. ORBITA-2 then removed background antianginal therapy and found a clearer signal: in patients with stable angina receiving little or no antianginal medication and coronary stenoses causing ischemia, PCI resulted in a lower angina symptom score than a placebo procedure, with a lower daily frequency of angina episodes and roughly three times the odds of becoming angina free at 12 weeks compared with placebo [15].
The composite picture from COURAGE, ISCHEMIA, ORBITA, and ORBITA-2 is that in stable coronary disease without high risk anatomy (left main, severe multivessel disease, or depressed ejection fraction), revascularization’s principal, reproducibly demonstrable benefit is angina relief, not a reduction in hard events, a distinction physiological lesion assessment cannot resolve on its own, because FFR/iFR indicate whether a lesion is flow limiting, not whether revascularizing it will change survival.
Microvascular and vasospastic disease: when the epicardial arteries are not the answer
A substantial fraction of patients with angina have no obstructive epicardial disease on angiography. The CorMicA trial was the first randomized trial to show that invasive coronary function testing, measuring FFR, CFR, and IMR together, could stratify and guide treatment in this population [19]. All patients underwent invasive testing of FFR, CFR, and IMR, and were randomly assigned to either stratified medical therapy based on the test results or to management with results withheld; in the intervention group, results were used to classify patients as having microvascular angina, vasospastic angina, both, or neither. The stratified approach produced a clinically meaningful benefit: a mean improvement of 11.7 units in the Seattle Angina Questionnaire summary score at 6 months (95% CI 5.0 to 18.4, P=0.001), alongside improvements in quality of life scores [19].
This pathway is conceptually distinct from, and complementary to, epicardial physiology. Diagnosis of angina has traditionally focused on detecting obstructive epicardial CAD to guide revascularization, but ORBITA and the CIAO substudy of ISCHEMIA have prompted renewed attention to causes of angina beyond obstructive disease. In practice, CFR/IMR testing is reserved for patients in whom epicardial stenoses have already been excluded or judged non obstructive but ischemia or anginal symptoms persist.
Summary comparison of physiological indices
| Index | Measurement basis | Hyperemia required | Pressure wire required | Validated ischemic cutoff | Key supporting evidence | Current guideline status (2024 ESC CCS) |
|---|---|---|---|---|---|---|
| Fractional Flow Reserve (FFR) | Ratio of mean distal coronary pressure (Pd) to mean aortic pressure (Pa) during maximal hyperemia | Yes (IV or IC adenosine) | Yes | ≤0.80 (gray zone 0.75–0.80) | DEFER (2001, 15-yr FU 2015); FAME (2009); FAME 2 (2012, 5-yr 2018, 11-yr 2026); FAME 3 (2022) | Class IA reference standard for intermediate, non-left-main stenoses |
| Instantaneous Wave-Free Ratio (iFR) / other NHPRs (Pd/Pa, dPR) | Resting Pd/Pa ratio during the diastolic wave-free period (iFR) or whole-cycle/diastolic resting ratio (Pd/Pa, dPR) | No | Yes | iFR ≤0.89; resting Pd/Pa and dPR similar thresholds | DEFINE-FLAIR (2017); iFR-SWEDEHEART (2017); 5-yr pooled analysis (2023, signal for higher mortality vs FFR) | Class IA, equally recommended alternative to FFR (cutoff ≤0.89) |
| Resting Full-Cycle Ratio (RFR) | Lowest Pd/Pa ratio identified anywhere across the entire cardiac cycle (not restricted to diastole) | No | Yes | ≤0.89 (diagnostically near-equivalent to iFR; gray zone ~0.86–0.93 vs FFR) | VALIDATE-RFR (2018); multiple RFR-vs-FFR concordance/meta-analysis studies | Considered an alternative resting (non-hyperemic) index alongside Pd/Pa, dPR |
| Coronary Flow Reserve (CFR) | Ratio of hyperemic to resting coronary blood flow velocity (Doppler) or thermodilution-derived flow, reflecting combined epicardial + microvascular capacity | Yes | Yes (Doppler or thermodilution guidewire) | <2.0 abnormal (commonly used threshold) | CorMicA (2018) — stratified medicine using CFR+IMR in ANOCA/INOCA | Recommended adjunct when microvascular disease (ANOCA/INOCA) suspected despite non-obstructive epicardial disease |
| Index of Microcirculatory Resistance (IMR) | Distal coronary pressure × hyperemic mean transit time, a thermodilution-derived estimate of minimal microvascular resistance | Yes | Yes (thermodilution-capable pressure wire) | ≥25 units abnormal (commonly used threshold) | CorMicA (2018); microvascular dysfunction literature post-MI and in INOCA | Recommended adjunct to CFR for microvascular endotyping in ANOCA/INOCA |
| Angiography-derived / wire-free FFR (QFR, FFRangio, vessel-FFR/3D-QCA) | Computational estimate of FFR from 3D quantitative coronary angiography ± modeled flow, without a physical pressure wire or (for most) pharmacologic hyperemia | No (model-derived; QFR uses assumed/derived hyperemic flow) | No | ≤0.80 (same threshold convention as wire-based FFR) | FAVOR III China (QFR, 2022/2024 outcome trial); ALL-RISE (FFRangio vs pressure wire, NEJM 2026, NCT05893498); FAST III (vessel-FFR/3D-QCA vs pressure wire, NEJM 2026, NCT04931771) | QFR: Class IA/IB (epicardial assessment, multivessel lesion selection); other vessel-FFR (e.g., FFRangio): Class IIb/C pending accumulating outcome data |
An integrated decision pathway
Figure 1 summarizes the evidence above into a single decision pathway, from an angiographically intermediate stenosis through choice of physiological index, the revascularization versus deferral decision, the symptom driven layer captured by ORBITA-2/ISCHEMIA, and the parallel microvascular/vasospastic pathway for non obstructive disease.
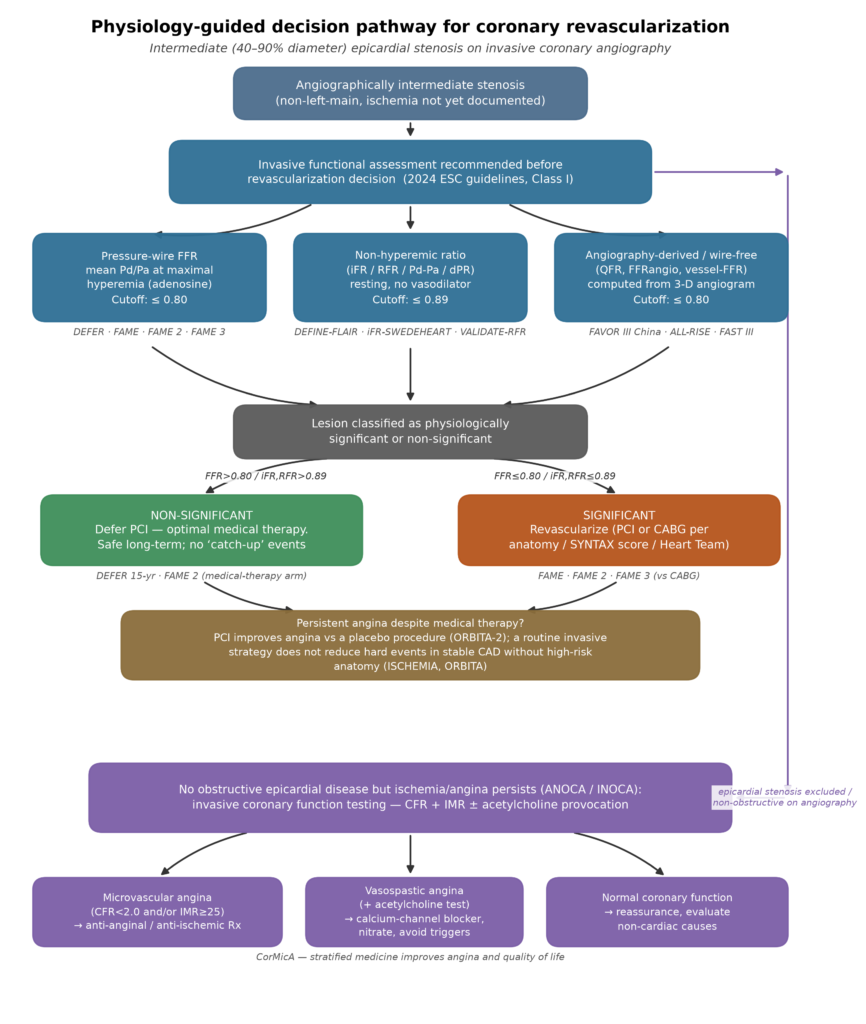
Figure 1. Physiology guided decision pathway for coronary revascularization, integrating epicardial physiological assessment (pressure wire FFR, non hyperemic resting indices, and angiography derived wire free indices), the deferral versus revascularization decision, the distinct question of symptom relief in patients on medical therapy, and the microvascular/vasospastic pathway for angina with non obstructive coronary arteries.
Future directions
Three trends define the current trajectory of this field. First, the procedural burden of physiological assessment has fallen steadily, from hyperemic, wire based FFR, to non hyperemic wire based indices (iFR, RFR), to fully angiography derived, wire free indices (QFR, FFRangio, vFFR), without, on the outcome evidence reviewed here, a corresponding loss of diagnostic or prognostic fidelity. ALL-RISE and FAST III are the clearest recent evidence for this trend, each showing noninferiority of an angiography derived index against pressure wire FFR itself (rather than against angiography alone), a materially higher evidentiary bar than earlier angiography derived validation studies cleared.
Second, the mortality signal in the pooled 5 year iFR versus FFR analysis is a reminder that 1 year noninferiority does not guarantee long term equivalence, and that the field should track long term outcomes for angiography derived indices with the same rigor once applied to iFR, the ALL-RISE and FAST III results reported here are 1 year outcomes, and their long term trajectories are not yet known.
Third, the revascularization versus medical therapy question and the physiological index selection question are separable but frequently conflated in clinical discussion. Physiological indices identify which lesions are hemodynamically significant; they do not, by themselves, establish that stenting a significant lesion will improve survival in a patient who is well controlled on medical therapy and free of high risk anatomy. The ISCHEMIA and ORBITA/ORBITA-2 data suggest the reliable, reproducible benefit of revascularization in this setting is angina relief, a conclusion that should temper any framing of physiological assessment as an unqualified gateway to more revascularization, rather than as (frequently) a gateway to safe deferral.
Finally, coronary microvascular and vasospastic disease remain comparatively under investigated relative to epicardial physiology, despite affecting a large fraction of patients with angina and non obstructive coronary arteries. Wider adoption of CFR/IMR testing, informed by the stratified medicine model demonstrated in CorMicA, is a plausible next frontier for closing the diagnostic gap that a purely epicardial, FFR centric pathway leaves open.
References
- Bech GJ, De Bruyne B, Pijls NHJ, et al. Fractional flow reserve to determine the appropriateness of angioplasty in moderate coronary stenosis: a randomized trial. Circulation. 2001;103:2928 to 2934.
- Zimmermann FM, Ferrara A, Johnson NP, et al. Deferral vs. performance of percutaneous coronary intervention of functionally non significant coronary stenosis: 15 year follow up of the DEFER trial. Eur Heart J. 2015;36:3182 to 3188. doi:10.1093/eurheartj/ehv452
- Tonino PAL, De Bruyne B, Pijls NHJ, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213 to 224. doi:10.1056/NEJMoa0807611
- Pijls NHJ, Fearon WF, Tonino PAL, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease: 2 year follow up of the FAME study. J Am Coll Cardiol. 2010;56:177 to 184. doi:10.1016/j.jacc.2010.04.012
- van Nunen LX, Zimmermann FM, Tonino PAL, et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5 year follow up of a randomised controlled trial. Lancet. 2015;386:1853 to 1860.
- De Bruyne B, Pijls NHJ, Kalesan B, et al. Fractional flow reserve guided PCI versus medical therapy in stable coronary disease (FAME 2). N Engl J Med. 2012;367:991 to 1001. doi:10.1056/NEJMoa1205361
- Xaplanteris P, Fournier S, Pijls NHJ, et al. Five year outcomes with PCI guided by fractional flow reserve (FAME 2). N Engl J Med. 2018;379:250 to 259. doi:10.1056/NEJMoa1803538
- Collet C, Mahendiran T, Fearon WF, et al. Fractional flow reserve guided percutaneous coronary intervention versus medical therapy for stable coronary artery disease: long term results of the FAME 2 trial. Nat Med. 2026;32:318 to 324. doi:10.1038/s41591-025-04132-5
- Fearon WF, Zimmermann FM, De Bruyne B, et al. Fractional flow reserve guided PCI as compared with coronary bypass surgery (FAME 3). N Engl J Med. 2022;386:128 to 137. doi:10.1056/NEJMoa2112299
- Davies JE, Sen S, Dehbi HM, et al. Use of the instantaneous wave free ratio or fractional flow reserve in PCI (DEFINE-FLAIR). N Engl J Med. 2017;376:1824 to 1834. doi:10.1056/NEJMoa1700445
- Götberg M, Christiansen EH, Gudmundsdottir IJ, et al. Instantaneous wave free ratio versus fractional flow reserve to guide PCI (iFR-SWEDEHEART). N Engl J Med. 2017;376:1813 to 1823. doi:10.1056/NEJMoa1616540
- Eftekhari A, Holck EN, Westra J, et al. Instantaneous wave free ratio vs. fractional flow reserve and 5 year mortality: iFR-SWEDEHEART and DEFINE-FLAIR. Eur Heart J. 2023;44:4376 to 4384. doi:10.1093/eurheartj/ehad582
- Svanerud J, Ahn JM, Jeremias A, et al. Validation of a novel non hyperaemic index of coronary artery stenosis severity: the Resting Full cycle Ratio (VALIDATE RFR) study. EuroIntervention. 2018;14:806 to 814.
- Al Lamee R, Thompson D, Dehbi HM, et al. Percutaneous coronary intervention in stable angina (ORBITA): a double blind, randomised controlled trial. Lancet. 2018;391:31 to 40.
- Rajkumar CA, Foley MJ, Ahmed Jushuf F, et al. A placebo controlled trial of percutaneous coronary intervention for stable angina (ORBITA-2). N Engl J Med. 2023;389:2319 to 2330. doi:10.1056/NEJMoa2310610
- Maron DJ, Hochman JS, Reynolds HR, et al. Initial invasive or conservative strategy for stable coronary disease (ISCHEMIA). N Engl J Med. 2020;382:1395 to 1407. doi:10.1056/NEJMoa1915922
- Spertus JA, Jones PG, Maron DJ, et al. Health status outcomes with invasive or conservative care in coronary disease (ISCHEMIA). N Engl J Med. 2020;382:1408 to 1419. doi:10.1056/NEJMoa1916370
- Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease (COURAGE). N Engl J Med. 2007;356:1503 to 1516. doi:10.1056/NEJMoa070829
- Ford TJ, Stanley B, Good R, et al. Stratified medical therapy using invasive coronary function testing in angina: the CorMicA trial. J Am Coll Cardiol. 2018;72:2841 to 2855.
- Xu B, Tu S, Song L, et al. Angiographic quantitative flow ratio guided coronary intervention (FAVOR III China): a multicentre, randomised, sham controlled trial. Lancet. 2021;398:2149 to 2159. doi:10.1016/S0140-6736(21)02248-0
- Song L, Xu B, Tu S, et al. 2 year outcomes of angiographic quantitative flow ratio guided coronary interventions. J Am Coll Cardiol. 2022;80:2089 to 2101. doi:10.1016/j.jacc.2022.09.007
- Vrints C, Andreotti F, Koskinas KC, et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024;45:3415 to 3537. doi:10.1093/eurheartj/ehae177
- [User specified reference] Angiography derived fractional flow reserve to guide PCI (ALL-RISE trial). N Engl J Med. 2026. doi:10.1056/NEJMoa2600949. ClinicalTrials.gov NCT05893498.
- [User specified reference] Angiography based physiology to guide coronary revascularization (FAST III trial). N Engl J Med. 2026. doi:10.1056/NEJMoa2601841. ClinicalTrials.gov NCT04931771.
- Crystal GJ, Klein LW. Fractional flow reserve: physiological basis, advantages and limitations, and potential gender differences. Curr Cardiol Rev. 2015;11:209 to 219.
- Jeremias A, Kirtane AJ, Stone GW. A test in context: fractional flow reserve: accuracy, prognostic implications, and limitations. J Am Coll Cardiol. 2017;69:2748 to 2758. doi:10.1016/j.jacc.2017.04.019
- De Waard GA, Di Mario C, Lerman A, Serruys PW, Van Royen N. Instantaneous wave free ratio to guide coronary revascularisation: physiological framework, validation and differences from fractional flow reserve. EuroIntervention. 2017;13:450 to 458.
- Petraco R, Park JJ, Sen S, et al. Hybrid iFR FFR decision making strategy: implications for enhancing universal adoption of physiology guided coronary revascularisation. EuroIntervention. 2013;8:1157 to 1165.
- Kern MJ, Lerman A, Bech JW, et al. Physiological assessment of coronary artery disease in the cardiac catheterization laboratory: a scientific statement from the American Heart Association. Circulation. 2006;114:1321 to 1341.

