Coronary artery disease: On LDL cholesterol, dietary fat & statins
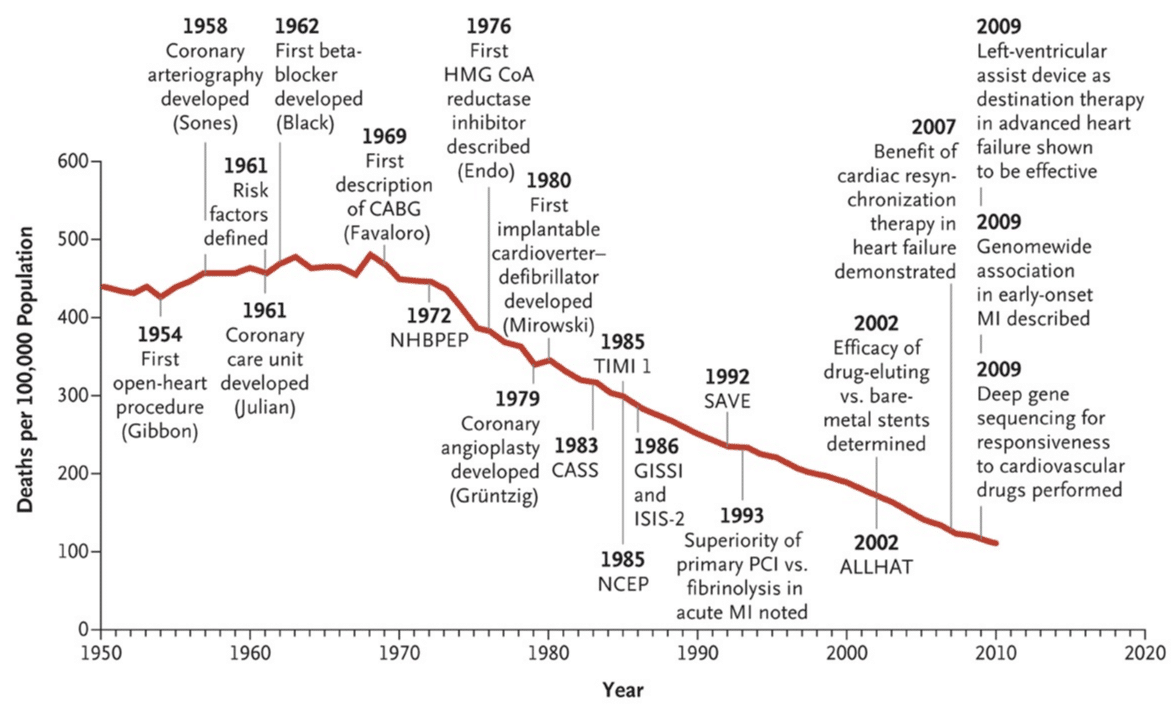
You are probably aware that ischemic heart disease, also known as coronary artery disease, has been the number one killer worldwide since the 1960s. In 1948 the NHLBI initiated the Framingham Heart Study, which demonstrated that high blood pressure and high cholesterol levels, among other risk factors, were strongly associated with coronary artery disease and myocardial infarction. However, association is not the same as causation. A cause is something completely different. It took roughly 50 years for researchers to finally conclude that high cholesterol levels caused coronary artery disease and atherosclerosis in general. This required thousands of observational studies, genetic studies and randomized controlled clinical trials. This knowledge has been translated into remarkable advances in the management of coronary artery disease, as demonstrated in the figure below (from Nabel et al, NEJM, 2014). In this post I would like to discuss hot topics related to coronary artery disease and I will emphasize on issues that are typically raised by patients.
The controversy: How media and bloggers questioned LDL, dietary fat and statins
Popular blogs and media reach out to billions of individuals worldwide. They exert enormous influence over their visitors daily lives. However, media outlets and bloggers are not necessarily experienced researchers, nor do they always take advice from experts (for whatever reason). LDL cholesterol, dietary fat and statins have been debated intensely in the past decade. A quick search (on Google) for anything related to statins, LDL cholesterol and dietary fat returns thousands of blogs and media posts that are skeptical of everything surrounding these topics. In the UK it was estimated that around 200.000 individuals stopped taking their statins after a study reported that there was no association between cholesterol and coronary artery disease in the elderly. That study spread like a virus through social media and it is likely that it may have resulted in increased mortality due to stopping statins. There are three main questions discussed in media, blogs and on social plattforms:
- Is high cholesterol a true cause of coronary artery disease?
- Does diet affect cholesterol levels?
- Are statins really effective, or is it all just a “big pharma” sham?
These are actually questions that patients tend to ask nowadays and therefore I will make an effort to clarify the issues.
Is high cholesterol levels a true cause of coronary artery disease?
First of all, don’t confuse various lipids, since they are extremely different with regards to their effects and hazards. For example, high HDL cholesterol levels appears to be beneficial, whereas triglyceride levels seem to be of little or no importance for atherosclerosis. When discussing atherosclerosis, the focus is on LDL cholesterol. Virtually all evidence demonstrate clearly that LDL cholesterol is a true cause of coronary artery disease. What is the evidence? The evidence is vast. Some examples follow. Consider people with the genetic disorder familial hypercholesterolemia (FH), which is caused by genetic mutations affecting the elimination of LDL cholesterol from the blood. Individuals with familial hypercholesterolemia may have either one defect gene copy (heterozygous FH) or two defect gene copies (homozygous FH). Heterozygous FH results in high LDL cholesterol levels (but nothing else) and increases the risk of acute myocardial infarction by more than 50 times. Individuals with homozygous FH typically die from acute myocardial infarction at 20 to 30 years of age. People with familial hypercholesterolemia have no other metabolic aberration, besides high LDL cholesterol. Treating these individuals with LDL lowering drugs, such as statins, reduces their risks markedly.
Epidemiological studies have consistently demonstrated that those with high LDL cholesterol levels are at increased risk of atherosclerotic disease, including coronary artery disease, acute myocardial infarction, stroke, peripheral artery disease etc. There are thousands of studies in this category.
A strong proof that LDL cholesterol causes myocardial infarction was obtained from clinical trials that evaluated the effect of lowering LDL cholesterol. These trials were mostly evaluating the effect of statins. There is no doubt that statins lowers the risk of acute myocardial infarction, coronary artery disease and stroke by means of lowering LDL cholesterol.
Finally, nature brought us another piece of strong evidence. There is a phenomenon in nature called “Mendelian Randomization”. For any given gene in the body there are 2 copies. These copies are inherited from our parents, which themselves also had 2 copies of each gene. Each of us has inherited 1 copy of each gene from each parent. Which ones we have inherited has actually been completely random. Hence, our 2 copies of each gene are actually a random selection of the 4 candidate genes our parents had. Some gene variants actually affect our physiology; for example some gene variants may result in diminished ability to clear LDL cholesterol from the blood stream, and thus cause elevated LDL cholesterol levels. We can use gene variants to study how they affect the risk of coronary artery disease, and that is done under the framework of Mendelian Randomization. Under laws of Mendelian Randomization, our genes are randomly assigned to us, which means that any effect of the gene variant will be a causal effect. Mendelian Randomization can therefore be used to decipher causal pathways. These studies also show, clearly, that high LDL cholesterol is a cause of coronary artery disease and atherosclerosis in general. In summary, there is no doubt that LDL cholesterol is a true cause of atherosclerosis.
But bloggers always say that LDL cholesterol is natural?
This is the oldest trick in the book. Certainly, LDL cholesterol is natural and thousands of species have LDL particles to deliver cholesterol to all tissues in the organism. However, the fact that LDL cholesterol is natural does not affect its tendency to accumulate within our coronary arteries. Unfortunately, bloggers often claim that LDL cholesterol cannot be hazardous because it is natural. This is false. To make the argument clear, consider potassium or thyroid hormone (T3, T4), which are both natural and abundant in our bodies. What occurs if potassium levels or thyroid hormone levels are doubled? Answer: you may actually die immediately if potassium levels go up twice, and a doubling of thyroid hormone levels would be very disturbing. Likewise, a doubling of LDL cholesterol also has negative effects; it accelerates the atherosclerotic process in our coronary arteries and elsewhere. Thus, the notion that LDL cannot be hazardous because its natural is false.
What about food? Does diet affect LDL cholesterol?
We used to believe that diet has a large effect of LDL cholesterol. More specifically, we believed that saturated fats were capable of elevating LDL cholesterol. This is probably not true and recent research have questioned the long standing notion that dietary fat has a significant effect on LDL cholesterol. Likewise, it seems that there is no association between dietary fat and risk of acute myocardial infarction. So in summary: no, dietary fat does not seem to have any considerable impact on blood fats (notably LDL cholesterol) nor the risk of acute myocardial infarction. Thus, don’t mix blood fats with dietary fats, there is simply no strong correlation.
Are statins effective? Big pharma is making so much money…
Despite the criticism, the pharmaceutical industry has financed clinical trials which have saved millions of lives and the statin trials are some of the most important trials ever conducted. I urge you to read Dr Collin’s and Dr Yusufs’ review of the statin trials. Briefly, statins are effective and they reduce the risk of myocardial infarction and cardiovascular disease. Statins cost approximately $3 per month and generic drugs are available worldwide. Many researchers are, however, concerned that the pharmaceutical companies have refused to release data from the statin trials, so that data on side effects can be better evaluated. I agree and wish that key data from clinical trials should be made publicly available. People at risk of acute myocardial infarction should are strong candidates for statin treatment.
As a final remark I would like to note that despite the many flaws in media and blog posts, it is absolutely right that there is public debate about the benefits and harms of treatments and clinical management.
Dr Araz Rawshani, MD, PhD
Institute of Medicine, Department of Molecular and Clinical Medicine
University of Gothenburg, Sweden
Published: 2018-03-23
Conflict of interest: None

