Cardiovascular effects of COVID-19
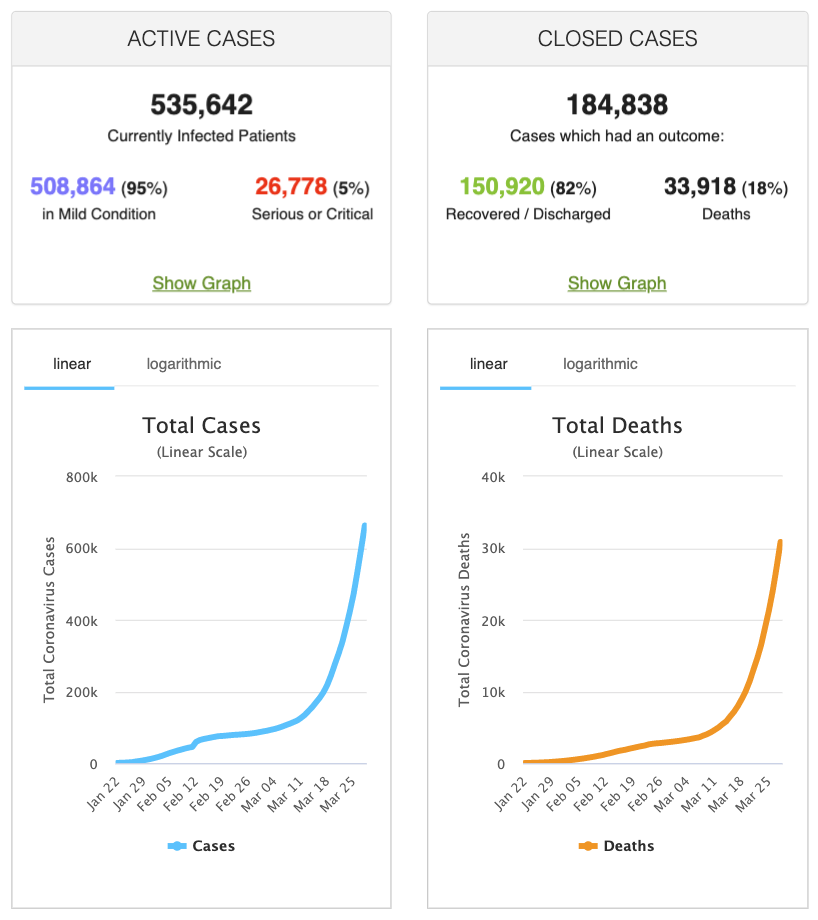
Coronavirus disease 2019 (COVID-19) has caused a global public health crisis. It is believed that the virus was transmitted from bats to humans in Wuhan, China, and it has now spread to more than 170 countries and caused unprecedented damage to humans and societies. The number of confirmed cases is approaching one million and the number of deaths is 34,000 as of March 29, 2020 (Figure 1). There are no known effective treatments, although several randomized controlled trials are underway.
Cardiovascular implications of COVID-19
Data on the natural history of COVID-19 relies on small samples of hospitalized patients. Most reports have suggested that comorbidities – e.g. cardiovascular disease, pulmonary disease, advanced age, smoking, diabetes, hypertension, cancer, etc – are the most important risk factors for poor outcomes. The vast majority of infections with COVID-19 result in mild disease, with symptoms similar to seasonal flu (influenza) and other viral respiratory infections. However, in some individuals the infection may be severe and deadly. Importantly, COVID-19 has caused an unprecedented number of severe and deadly infections among young and apparently healthy individuals.
Infections and the risk of acute coronary syndromes
It is known that the risk of developing acute coronary syndromes increases during infections, including influenza (6–9). Two mechanisms have been proposed to precipitate acute coronary events during infections:
- An acute coronary event may be triggered by increased myocardial demand during the infection.
- Systemic inflammation results in increased levels of circulating pro-inflammatory cytokines that may cause plaque rupture (i.e the risk of atherosclerotic plaque rupture is increased during infections).
As noted by Bonow et al, it is also reasonable to believe that patients with heart failure are at increased risk of decompensation if infected with COVID-19. Moreover, there may also be an increased risk of myocarditis, given the similarities between COVID-19 and MERS (Middle East Respiratory Syndrome, coronavirus).
Recent studies on COVID-19 and cardiovascular disease
Cardiovascular implications of COVID-19 have been elucidated in recent studies from China and Italy (1–5). Two recent studies published in JAMA Cardiology are summarized below.
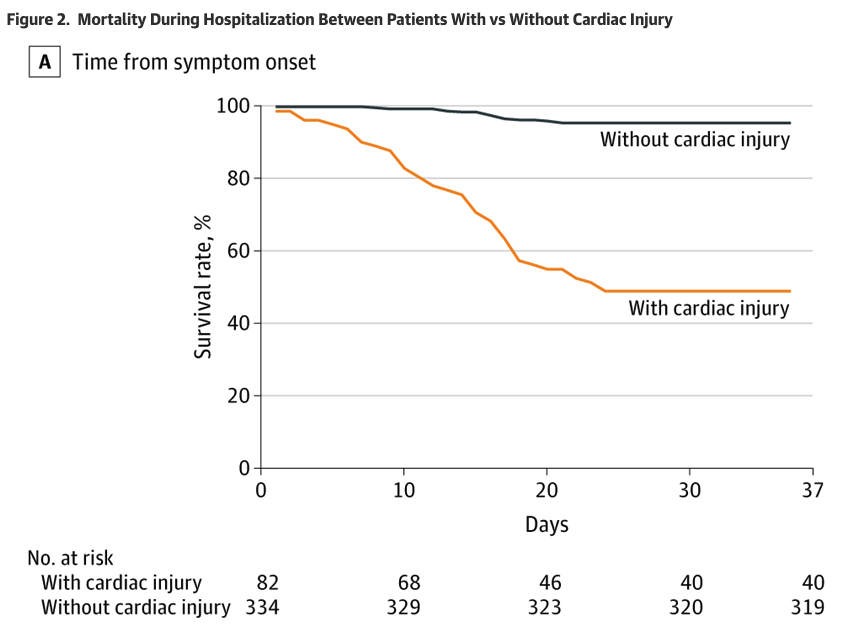
Shi et al present data on 416 patients hospitalized with COVID-19. In total, 82 patients (19.7%) had elevated high-sensitivity troponin I (TnI) levels. The mortality rate among patients with elevated troponin I was 51.2%, as compared with 4.5% among patients without evidence of myocardial injury (normal troponin I levels). Hence, troponin I was a strong predictor of survival in patients hospitalized with COVID-19 (Figure 2).
Guo et al reported that 27.8% (52 of 187 patients) had myocardial injury, defined as elevated troponin T levels (TnT). In-hospital mortality rate was 59.6% among cases with elevated TnT levels, as compared with 8.9% among patients with normal TnT levels. Increased risk of death was noted among all patients with elevated troponin levels, although the highest risk was noted among patients with cardiovascular disease. The highest mortality rate was observed in patients with elevated TnT levels who had underlying cardiovascular disease, of which 69.4% died.
Guo et al also report a significant association between troponin T levels and C-reactive protein (CRP) and N-terminal pro-B-type natriuretic peptide (NT-pro-BNP). The latter suggests that COVID-19 causes ventricular dysfunction. Guo et al also demonstrate that troponin T and NT-pro-BNP may be used as prognostic markers during the disease course.
In summary, the risk of severe disease and death is several times higher in patients with cardiovascular disease. This suggests that every effort must be made to prevent COVID-19 transmission to individuals with cardiovascular conditions.
For details, refer to the excellent editorial by Bonow et al.
References
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506.
- Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507-513.
- Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061-1069.
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA.
- Guan WJ, Ni ZY, Hu Y, et al; China Medical Treatment Expert Group for Covid-19. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. Published online February 28, 2020.
- Madjid M, Miller CC, Zarubaev VV, et al. Influenza epidemics and acute respiratory disease activity are associated with a surge in autopsy-confirmed coronary heart disease death: results from 8 years of autopsies in 34,892 subjects. Eur Heart J. 2007;28(10):1205-1210.
- Nguyen JL, Yang W, Ito K, Matte TD, Shaman J, Kinney PL. Seasonal influenza infections and cardiovascular disease mortality. JAMA Cardiol. 2016;1(3):274-281.
- Kwong JC, Schwartz KL, Campitelli MA, et al. Acute myocardial infarction after laboratory-confirmed influenza infection. N Engl J Med. 2018;378(4):345-353.
- Smeeth L, Thomas SL, Hall AJ, Hubbard R, Farrington P, Vallance P. Risk of myocardial infarction and stroke after acute infection or vaccination. N Engl J Med. 2004;351(25):2611-2618.
- Shi S, Qin M, Shen B, et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. Published online March 25, 2020.
- Guo T, Fan Y, Chen M, et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. Published online March 27, 2020.

